Treatment in Pediatric Renal Trauma: A Conservative Management Approach
- Affiliations
-
- 1Department of Urology, College of Medicine, Inje University, Seoul, Koreae. chungj90@paran.com
Abstract
- PURPOSE
The management of pediatric trauma is substantially derived from the results of adult trauma patient. Despite the increasing of pediatric renal trauma, the management of them still remains controversial. The aim of this study is to evaluate our experience with the expectant conservative management of blunt trauma in children.
MATERIALS AND METHODS
We retrospectively studied 45 pediatric patients with renal trauma between 1995 and 2007. We reviewed medical records for clinical symptoms, mechanism of injury, assigned grade of renal injury, associated injuries, indication of surgery, and treatment outcomes. We graded renal injuries according to the American Association for the Surgery of Trauma Organ Injury Scale.
RESULTS
All patients of grade I, II, III, and IV were managed conservatively at beginning, if the hemodynamic state is stable. Among them, 2 patients of grade IV were done delayed operation. One patient underwent delayed renorrhaphy for persistent anemia and hypotension, and the other patient needed delayed nephrectomy because of persistent fever and worsening abdominal pain with significant urinary extravasation. All patients of grade V were undergone early nephrectomy.
CONCLUSIONS
Except for persistent fever with significant extravasation and grade V injury, initial conservative management of blunt renal trauma in children is effective and recommendable at beginning, if the hemodynamic state is stable. Prospective larger randomized controlled trials will be needed.
Keyword
MeSH Terms
Figure
-

Fig. 1 Radiographic appearance of grade IV right renal injury in a 4-year-old child whose conservative treatment was failed. (A) Computerized tomography (CT) presents deep lacerations with main vascular injury of right kidney. (B) CT shows well healed kidney after 3 months from renorrhaphy.
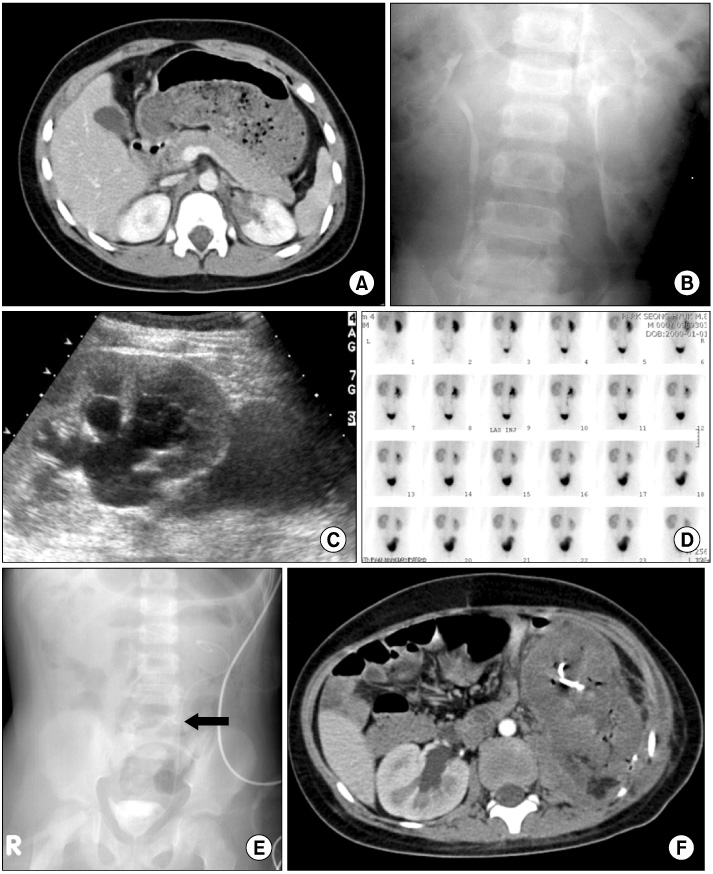
Fig. 2 Eight-year-old child with blunt renal trauma. (A, B) On admission, computerized tomography (CT) shows perinephric extravasation of contrast media from left upper collecting system. (C) Follow-up sonography 4 weeks later presents new developed hydronephrosis and increased perinephric urinoma. (D) Diethylenetriaminepentaacetic acid (DTPA) lasix renal scan image 5 weeks after injury shows relative delay in clearance from the left kidney and demonstrates relatively decreased renal function. (E) At 7 weeks after injury, ureteral stenting was done. (F) CT shows infarction of left kidney just before nephrectomy.
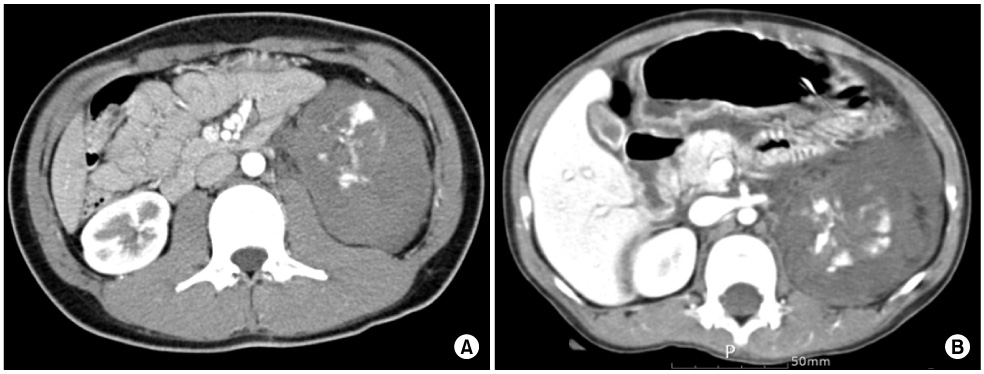
Fig. 3 Computerized tomography (CT) scan showing a grade V traumatic injury of left kidney each other. (A) 14-year-old boy, (B) 6-year-girl, transverse section image showing the shattered renal parenchyma of mid pole kidney. Early nephrectomy was required in all patients.
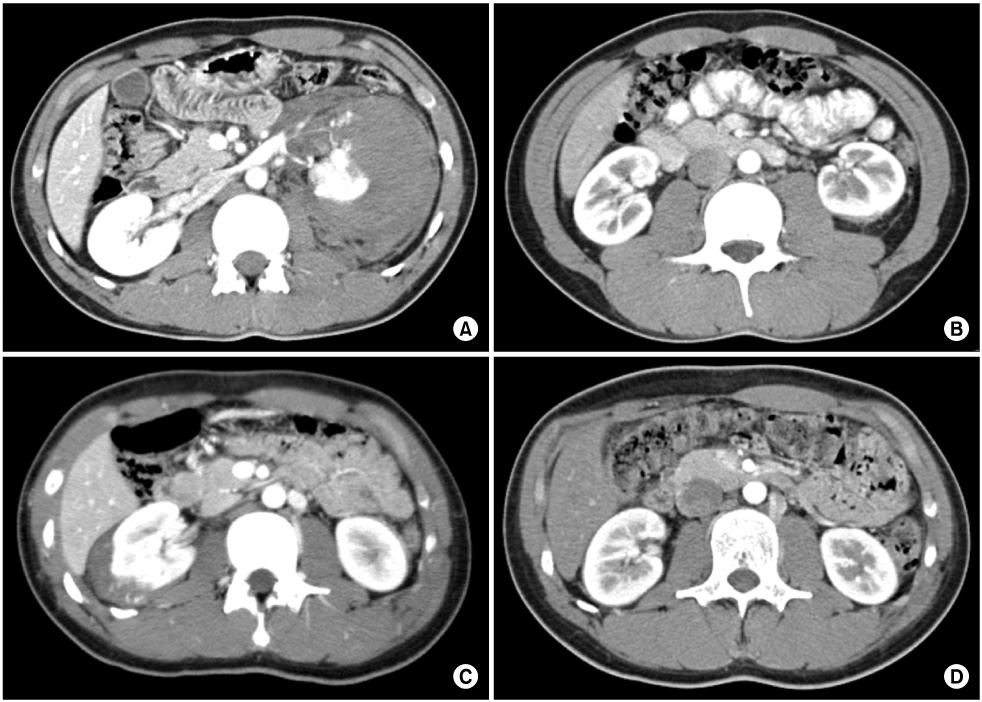
Fig. 4 The durations of improvement was longer in the higher grade injury comparing the lower grade one in follow-up images. (A, B) Parenchymal lacerations and amount of hematoma were resolved in 3 months after grade IV injury. (C, D) Perirenal hematoma was resolved completely in 4 weeks after grade III injury.
Reference
-
1. American Academy of Pediatrics Section on Orthopaedics; American Academy of Pediatrics Committee on Pediatric Emergency Medicine; American Academy of Pediatrics Section on Critical Care; American Academy of Pediatrics Section on Surgery; American Academy of Pediatrics Section on Transport Medicine; American Academy of Pediatrics Committee on Pediatric Emergency Medicine, et al. Management of pediatric trauma. Pediatrics. 2008. 121:849–854.2. Kim DH, Lee SH, Lee SB, Ryu MH, Lee DJ. Clinical analysis of pediatric death patients visiting emergency center. Korean J Pediatr. 2004. 47:12–17.3. Livne PM, Gonzales ET Jr. Genitourinary trauma in children. Urol Clin North Am. 1985. 12:53–65.4. Wessel LM, Scholz S, Jester I, Arnold R, Lorenz C, Hosie S, et al. Management of kidney injuries in children with blunt abdominal trauma. J Pediatr Surg. 2000. 35:1326–1330.5. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: spleen, liver, and kidney. J Truma. 1989. 29:1664–1666.6. Buckley JC, McAninch JW. Pediatric renal injuries: management guidelines from a 25-year experience. J Urol. 2004. 172:687–690.7. Brown SL, Elder JS, Spirnak JP. Are pediatric patients more susceptible to major renal injury from blunt trauma? A comparative study. J Urol. 1998. 160:138–140.8. Lee JH, Yoon SJ, Lee JB. Comparison of blunt renal injury between children and adults: effect of the causes on severity of renal injury. Korean J Urol. 2005. 46:32–36.9. Sahin H, Akay AF, Yilmaz G, Tacyildiz IH, Bircan MK. Retrospective analysis of 135 renal trauma cases. Int J Urol. 2004. 11:332–336.10. Miller KS, McAninch JW. Radiographic assessment of renal trauma: our 15-year experience. J Urol. 1995. 154:352–355.11. Morse TS. Renal injuries. Pediatr Clin North Am. 1975. 22:379–391.12. Chopra P, St-Vil D, Yazbeck S. Blunt renal trauma-blessing in disguise? J Pediatr Surg. 2002. 37:779–782.13. Morey AF, Bruce JE, McAninch JW. Efficacy of radiographic imaging in pediatric blunt renal trauma. J Urol. 1996. 156:2014–2018.14. Santucci RA, Langenburg SE, Zachareas MJ. Traumatic hematuria in children can be evaluated as in adults. J Urol. 2004. 171:822–825.15. Hammer CC, Santucci RA. Effect of an institutional policy of nonoperative treatment of grade I to IV renal injuries. J Urol. 2003. 169:1751–1753.16. Keller MS, Eric Coln C, Garza JJ, Sartorelli KH, Christine Green M, Weber TR. Functional outcome of nonoperatively managed renal injuries in children. J Trauma. 2004. 57:108–110.17. Heyns CF. Renal trauma: indications for imaging and surgical exploration. BJU Int. 2004. 93:1165–1170.18. Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW, et al. Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee. BJU Int. 2004. 93:937–954.19. Cass AS, Luxenberg M. Conservative or immediate surgical management of blunt renal injuries. J Urol. 1983. 130:11–16.20. Santucci RA, McAninch JW, Safir M, Mario LA, Service S, Segal MR. Validation of the American Association for the Surgery of Trauma organ injury severity scale for the kidney. J Trauma. 2001. 50:195–200.21. Husmann DA, Gilling PJ, Perry MO, Morris JS, Boone TB. Major renal lacerations with a devitalized fragment following blunt abdominal trauma: a comparison between nonoperative (expectant) versus surgical management. J Urol. 1993. 150:1774–1777.22. Russell RS, Gomelsky A, McMahon DR, Andrews D, Nasrallah PF. Management of grade IV renal injury in children. J Urol. 2001. 166:1049–1050.23. Rogers CG, Knight V, MacUra KJ, Ziegfeld S, Paidas CN, Mathews RI. High-grade renal injuries in children-is conservative management possible? Urology. 2004. 64:574–579.24. Wessells H, McAninch JW, Meyer A, Bruce J. Criteria for nonoperative treatment of significant penetrating renal lacerations. J Urol. 1997. 157:24–27.25. Joung JY, Park SC, Kim JB, Kim HK, Park JY, Cheon SH, et al. Comparison of operative versus conservative management in pediatric renal trauma. Korean J Urol. 2005. 46:124–130.26. Altman AL, Haas C, Dinchman KH, Spirnak JP. Selective nonoperative management of blunt grade 5 renal injury. J Urol. 2000. 164:27–30.27. Kansas BT, Eddy MJ, Mydlo JH, Uzzo RG. Incidence and management of penetrating renal trauma in patients with multiorgan injury: extended experience at an inner city trauma center. J Urol. 2004. 172:1355–1360.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Renal embolization for trauma: a narrative review
- The Renal Angiography in Blunt Renal Trauma
- Comparison of Operative Versus Conservative Management in Pediatric Renal Trauma
- Conservative management of blunt major renal lacerations: risk factors versus the short-term and long-term complications
- Management of High-grade Blunt Renal Trauma
