Segmental Testicular Infarction: Radiologic Diagnosis and Conservative Management
- Affiliations
-
- 1Department of Urology, College of Medicine, Pusan National University, Busan, Korea. psw-ooz@hanmail.net
- 2Department of Radiology, College of Medicine, Pusan National University, Busan, Korea.
Abstract
- Segmental testicular infarction is a rare cause of an acute scrotum. The etiology can be related to sickle cell anemia, hypersensitivity angiitis and polycythemia in some cases, but the condition is usually an idiopathic phenomenon. Because making the differential diagnosis between segmental testicular infarction and testicular tumor can be difficult, most authors have recommended surgery in the past. We report here on cases of testicular segmental infarction that were treated by conservative management and we describe the radiologic findings.
Keyword
MeSH Terms
Figure
-

Fig. 1. Ultrasonography of the left testis. The lesion is hypoechoic, relatively well defined, rather nodular in shape and avascular (arrow).

Fig. 2. (A) Magnetic resonance imaging (MRI) of the testis. The T2-weight image shows a relatively well defined lesion on left testis (arrow). (B) MRI of the testis. The T1-weight image shows isointensity with some areas of hyperintensity within left testis, and this is suggestive of hemorrhage (arrow). (C) On the postcontrast T1-weighted MRI, the lesion is hypointense, indicating no uptake of contrast in the lesion, and the borders of the infarct are clearly enhanced (enhancing rim-arrow).

Fig. 3. Ultrasonography of the left testis shows complete resolution.
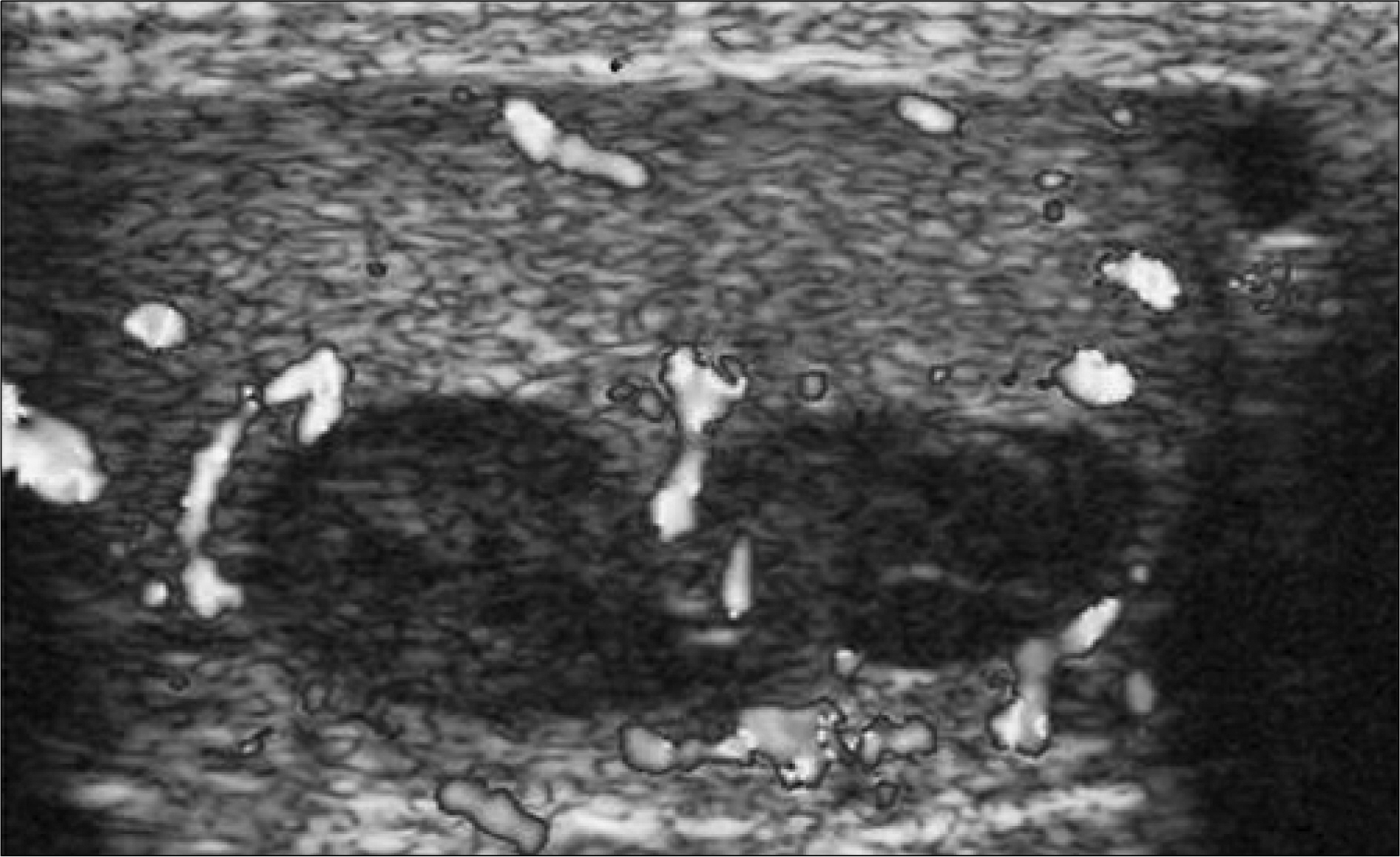
Fig. 4. Ultasonography of the right testis. The lesion is a well defined hypoechoic avascular lesion that has a snowman appearance.

Fig. 5. (A) On the T1-weighted magnetic resonance imaging (MRI), the lesion is hypointense, indicating no uptake of contrast in the lesion and the borders of the infarct are clearly enhanced. (B) MRI of the testis. The T2 image shows a relatively well defined lesion on the right testis (arrow). (C) The MR diffusion image shows the low signal intensity of the lesion that's due to the decreased diffusion.
Reference
-
1. Magill P, Jacob T, Lennon GM. A rare case of segmental testicular infarction. Urology. 2007; 69:983.
Article2. Nam JS, Kim DS, Lee ST, Lee YG, Cho ST, Kim KK. Segmental testicular infarction masquerading as testicular neoplasm. Korean J Urol. 2005; 46:1228–30.3. Sidhu PS. Clinical and imaging features of testicular torsion: role of ultrasound. Clin Radiol. 1999; 54:343–52.
Article4. Jordan GH. Segmental hemorrhagic infacrt of testicle. Urology. 1987; 29:60–3.5. Madaan S, Joniau S, Klockaerts K, Dewever L, Lerut E, Oyen R, et al. Segmental testicular infarction: conservative management is feasible and safe. Eur Urol. 2008; 53:441–5.
Article6. Ruibal M, Quintana JL, Fernandex G, Zungri E. Segmental testicular infarction. J Urol. 2003; 170:187–8.
Article7. Fernandez-Perez GC, Tardaguila FM, Velasco M, Rivas C, Dos Santos J, Cambronero J, et al. Radiologic findings of segmental testicular infarction. AJR Am J Roentgenol. 2005; 184:1587–93.8. Sriprasad S, Kooiman GG, Muir GH, Sidhu PS. Acute segmental testicular infarction: differentiation from tumour using high frequency colour Doppler ultrasound. Br J Radiol. 2001; 74:965–7.
Article9. Cramer BW, Schlegel EA, Thueroff JW. MR imaging in the differential diagnosis of scrotal and testicular disease. Radio-graphics. 1991; 11:9–21.
Article10. Kodama K, Yotsuyanagi S, Fuse H, Hirano S, Kitagawa K, Masuda S. Magnetic resonance imaging to diagnose segmental testicular infarction. J Urol. 2000; 163:910–1.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Unusual Case of Testicular Seminoma Mimicking Segmental Testicular Infarction
- Segmental Testicular Infarction Masquerading as Testicular Neoplasm
- Segmental Testicular Infarction Treated with Partial Orchiectomy
- Shear-Wave Elastography of Segmental Infarction of the Testis
- Various Intratesticular Hypoechoic Lesions on Scrotal Sonography
