A Case of Anorexia Nervosa Complicated With Strongly Suspected Stress-Induced Cardiomyopathy and Mural Thrombus
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. younhj@catholic.ac.kr
- KMID: 2297922
- DOI: http://doi.org/10.4070/kcj.2011.41.10.615
Abstract
- Stress-induced cardiomyopathy is a unique reversible cardiovascular disease precipitated by acute emotional or physical stress. It is associated with a high prevalence of chronic anxiety disorder that precedes the onset of cardiomyopathy, as well as comorbid cardiovascular risk factors that are similar to the ST segment elevation of myocardial infarction. A thirty-five-year-old woman suffering from anorexia nervosa visited our hospital complaining of severe general weakness. She was diagnosed with stress-induced cardiomyopathy and mural thrombus using a transthoracic echocardiogram. Therefore, she was given anticoagulation therapy and nutrition with immediate psychiatric interventions. After two weeks of treatment, the follow-up echocardiogram indicated a significant improvement of the left ventricular dysfunction and mural thrombus.
Keyword
MeSH Terms
Figure
-
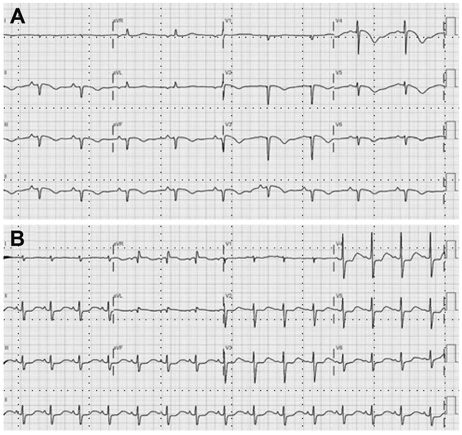
Fig. 1 Electrocardiogram on admission and follow-up. A: the electrocardiogram revealed significant QTc prolongation and T wave inversion in leads II, III, aVF and V1-V6 on admission day. It also showed pathologic Q wave in leads II, III, aVF and V1-V3. B: follow-up electrocardiogram revealed normal sinus rhythm with non-specific ST segment change on the 7th hospital day.
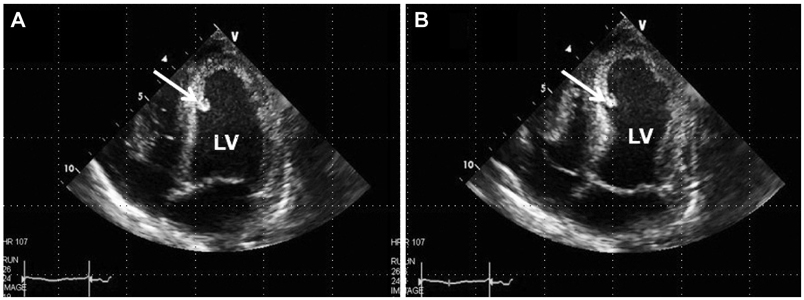
Fig. 2 Transthoracic echocardiogram on admission. A: the photograph demonstrates a large akinetic area around the apex during diastole with linear echogenic mural thrombus (arrow) surrounding septal apex. B: this photograph showed hypercontraction of the basal segments with reduction of ejection fraction to 36% during systole.
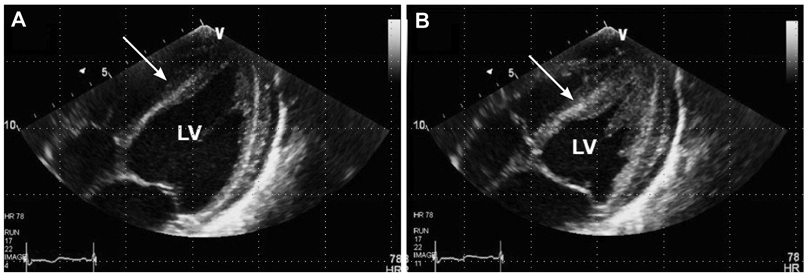
Fig. 3 Follow-up transthoracic echocardiogram. A: the previous akinetic left ventricular walls showed an improvement on the wall motion during diastole, and the mural thrombus decreased (arrow). B: during systole, the improvement of the systolic left ventricular function was noticed: ejection fraction increased to 59% and pericardial effusion increased.
Reference
-
1. Morris J, Twaddle S. Anorexia nervosa. BMJ. 2007. 334:894–898.2. Satoh H, Tateishi H, Uchida T. Kodama K, Haze K, Hon M, editors. Takotshubo-type cardiomyopathy due to multivessel spasm. Clinical Aspect of Myocardial Injury: from Ischemia to Heart Failure. 1990. Tokyo: Kagakuhyouronsya;56–64.3. Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol. 2001. 38:11–18.4. Saito S, Kita K, Morioka CY, Watanabe A. Rapid recovery from anorexia nervosa after a life-threatening episode with severe thrombocytopenia: report of three cases. Int J Eat Disord. 1999. 25:113–118.5. Isner JM, Roberts WC, Heymsfield SB, Yager J. Anorexia nervosa and sudden death. Ann Intern Med. 1985. 102:49–52.6. Cooke RA, Chambers JB. Anorexia nervosa and the heart. Br J Hosp Med. 1995. 54:313–317.7. Mont L, Castro J, Herreros B, et al. Reversibility of cardiac abnorma-lities in adolescents with anorexia nervosa after weight recovery. J Am Acad Child Adolesc Psychiatry. 2003. 42:808–813.8. Ohwada R, Hotta M, Kimura H, et al. Ampulla cardiomyopathy after hypoglycemia in three young female patients with anorexia nervosa. Intern Med. 2005. 44:228–233.9. Rotondi F, Manganelli F, Lanzillo T, et al. Tako-tsubo cardiomyopathy complicated by recurrent torsade de pointes in a patient with anorexia nervosa. Intern Med. 2010. 49:1133–1137.10. Haghi D, Papavassiliu T, Heggemann F, Kaden JJ, Corggrefe M, Suselbeck T. Incidence and clinical significance of left ventricular thrombus in tako-tsubo cardiomyopathy assessed with echocardiography. QJM. 2008. 101:381–386.11. Elesber AA, Prasad A, Lennon RJ, Wright RS, Lerman A, Rihal CS. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J Am Coll Cardiol. 2007. 50:448–452.12. Hong KS. Stress-induced cardiomyopathy: a need for rospective multicenter trials. Korean Circ J. 2010. 40:258–259.13. Lee HH, Gwon HC, Kim BJ, et al. Clinical manifestation of novel stress-induced cardiomyopathy mimicking acute myocardial infarction. Single center prospective registry. Korean Circ J. 2002. 32:1054–1063.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Ventricular Thrombus Associated with Takotsubo Cardiomyopathy: A Cardioembolic Cause of Cerebral Infarction
- Successful Treatment of Anorexia Nervosa in a 10-year-old Boy with Risperidone Long-acting Injection
- Surgical Removal of a Left Ventricular Thrombus Which Showed Morphologic Changes Over Time in a Patient with Stress-Induced Cardiomyopathy
- Inpatient Treatment of Anorexia Nervosa: Clinical Practice Models
- Pericardial effusion in three cases of anorexia nervosa
