J Clin Neurol.
2012 Mar;8(1):83-86. 10.3988/jcn.2012.8.1.83.
A Case of Cluster Headache Accompanied by Myoclonus and Hemiparesis
- Affiliations
-
- 1Department of Neurology, Gachon University Gil Hospital, Incheon, Korea. neurohm@gilhospital.com
- KMID: 2287623
- DOI: http://doi.org/10.3988/jcn.2012.8.1.83
Abstract
- BACKGROUND
Cluster headache is a primary headache disorder characterized by periodic episodes of intense headache accompanied by autonomic symptoms. We report an unusual clinical presentation of cluster headache that was preceded by myoclonus and accompanied by hemiparesis.
CASE REPORT
A 26-year-old man visited hospital due to recurrent jerky movements on the left side of his face and neck area lasting 3 days. These jerky movements had disappeared spontaneously without specific treatment. On the 10th day after onset of the jerky movements, the patient developed a series of unilateral severe headaches that were accompanied by autonomic symptoms lasting 1-2 hours. According to the second edition of The International Classification of Headache Disorders, he was diagnosed as having cluster headache. Two of the 16 severe headache attacks this patient suffered were accompanied by dysarthria and hemiparesis. Electroencephalography performed during hemiparesis revealed diffuse lateralized slow activity on the ipsilateral hemisphere of the headache side. The headache and accompanying hemiparesis disappeared after medical treatment for cluster headache.
CONCLUSIONS
We describe a case of cluster headache accompanied by hemiparesis, which was preceded by myoclonus. We also outline the possible mechanisms underlying this case.
MeSH Terms
Figure
-
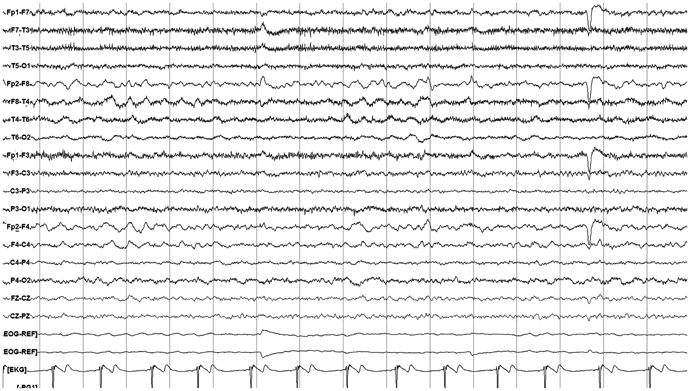
Fig. 1 A 24-hour video-monitoring electroencephalography showing lateralized slowing on the right hemisphere, beginning 20 minutes prior to the head-ache attack.
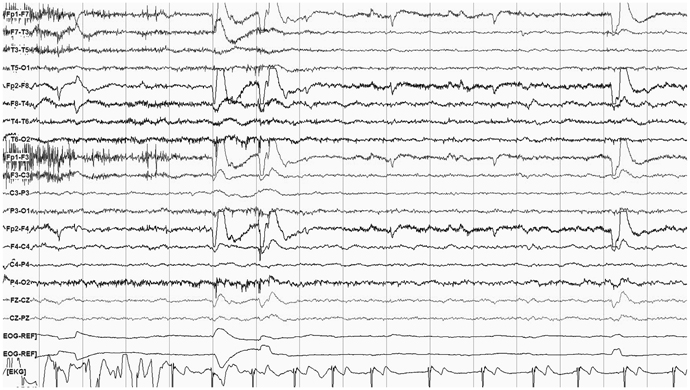
Fig. 2 A 24-hour video-monitoring electroencephalography showing normalization after headache relief.
Reference
-
1. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004. 24:Suppl 1. 9–160.2. Siow HC, Young WB, Peres MF, Rozen TD, Silberstein SD. Hemiplegic cluster. Headache. 2002. 42:136–139.
Article3. Langedijk M, van der Naalt J, Luijckx GJ, De Keyser J. Cluster-like headache aura status. Headache. 2005. 45:80–81.
Article4. Krymchantowski AV. Aura with non-migraine headache. Curr Pain Headache Rep. 2005. 9:264–267.
Article5. Goadsby PJ. Pathophysiology of cluster headache: a trigeminal autonomic cephalgia. Lancet Neurol. 2002. 1:251–257.
Article6. May A. Cluster headache: pathogenesis, diagnosis, and management. Lancet. 2005. 366:843–855.
Article7. Ramagopalan SV, Ramscar NE, Cader MZ. Molecular mechanisms of migraine? J Neurol. 2007. 254:1629–1635.
Article8. Rogawski MA. Common pathophysiologic mechanisms in migraine and epilepsy. Arch Neurol. 2008. 65:709–714.
Article9. Bolay H, Reuter U, Dunn AK, Huang Z, Boas DA, Moskowitz MA. Intrinsic brain activity triggers trigeminal meningeal afferents in a migraine model. Nat Med. 2002. 8:136–142.
Article10. Marshall WH. Spreading cortical depression of Leao. Physiol Rev. 1959. 39:239–279.11. Sand T. EEG in migraine: a review of the literature. Funct Neurol. 1991. 6:7–22.12. Varkey B, Varkey L. EEG in hemiplegic migraine. Neurol India. 2004. 52:134.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cluster-like Headache Secondary to Cerebral Venous Thrombosis
- Efficacy of Antiviral Treatment for Herpes-associated Erythema Multiforme Accompanied by Cluster Headache
- Acute Lymphocytic Leukemia of Periorbital Tissue Presenting with Cluster-Like Headache
- Pulsed Radiofrequency of the Sphenopalatine Ganglion for Treatment of a Cluster Headache: A case report
- Prevention with 240 mg Galcanezumab of Episodic Cluster Headache
