Chonnam Med J.
2012 Apr;48(1):39-46. 10.4068/cmj.2012.48.1.39.
Is Myocardial Infarction in Patients without Significant Stenosis on a Coronary Angiogram as Benign as Believed?
- Affiliations
-
- 1Department of Cardiology, Chonnam National University Hospital, Gwangju, Korea. cecilyk@hanmail.net
- KMID: 2274880
- DOI: http://doi.org/10.4068/cmj.2012.48.1.39
Abstract
- The present study aimed to investigate the clinical characteristics and 1-year outcomes of acute myocardial infarction (AMI) patients without significant stenosis on a coronary angiogram comparison with the clinical characteristics and outcomes of patients with significant coronary artery stenosis. A total of 1,220 patients with AMI were retrospectively classified into Group I (> or =50% diameter stenosis, n=1,120) and Group II (<50%, n=100). Group II was further divided into two subgroups according to the underlying etiology: cryptogenic (Group II-a, n=54) and those with possible causative factors (Group II-b, n=46). Patients in Group II were younger, were more likely to be women, and were less likely to smoke and to have diabetes mellitus than were patients in Group I. The levels of cardiac enzymes, LDL-cholesterol levels, and the apo-B/A1 ratio were lower in Group II. However, 1-month and 12-month rates of major adverse cardiac events (MACE) were not significantly different between the two groups. The Group II-b subgroup comprised 29 patients with vasospasm, 11 with myocardial bridge, and 6 with spontaneous thrombolysis. Left ventricular ejection fraction and creatinine clearance were lower and levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) and high-sensitivity C-reactive protein (hs-CRP) were higher in Group II-a than in Group II-b. However, outcomes including MACE and mortality at 12 months were not significantly different between the two subgroups. The 1-year outcomes of patients in Group II were similar to those of patients in Group I. The clinical outcomes in Group II-a were also similar to those of Group II-b, although the former group showed higher levels of NT-proBNP and hs-CRP.
MeSH Terms
Figure
-
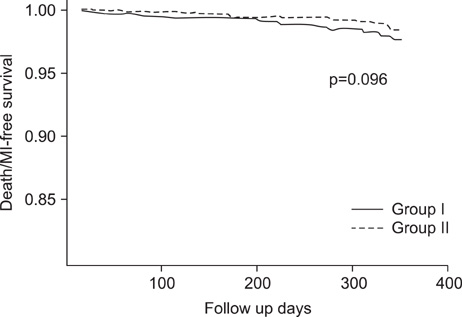
FIG. 1 Kaplan-Meir plots of cumulative death or myocardial infarction-free survival for patients with acute myocardial infarction with (Group I, n=1,120) or without (Group II, n=100) significant coronary stenosis. There was a trend for a lower incidence of death or myocardial infarction in Group II than in Group I during 1 year of clinical follow-up (p=0.096).
Reference
-
1. Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation. 2001. 104:365–372.
Article2. Legrand V, Deliege M, Henrard L, Boland J, Kulbertus H. Patients with myocardial infarction and normal coronary arteriogram. Chest. 1982. 82:678–685.
Article3. Negus BH, Willard JE, Glamann DB, Landau C, Snyder RW 2nd, Hillis LD, et al. Coronary anatomy and prognosis of young, asymptomatic survivors of myocardial infarction. Am J Med. 1994. 96:354–358.
Article4. Kardasz I, De Caterina R. Myocardial infarction with normal coronary arteries: a conundrum with multiple aetiologies and variable prognosis: an update. J Intern Med. 2007. 261:330–348.
Article5. Fuster V, Chesebro JH, Frye RL, Elveback LR. Platelet survival and the development of coronary artery disease in the young adult: effects of cigarette smoking, strong family history and medical therapy. Circulation. 1981. 63:546–551.
Article6. Ross R, Kay R, Ambrose J, Herman MV. Coronary thrombosis in the absence of angiographically-evident obstructive coronary disease. Chest. 1983. 84:768–770.
Article7. Steele P, Rainwater J, Vogel R. Abnormal platelet survival time in men with myocardial infarction and normal coronary arteriogram. Am J Cardiol. 1978. 41:60–62.
Article8. Gersh BJ, Bassendine MF, Forman R, Walls RS, Beck W. Coronary artery spasm and myocardial infarction in the absence of angiographically demonstrable obstructive coronary disease. Mayo Clin Proc. 1981. 56:700–708.9. Glazier JJ, McGinnity JG, Spears JR. Coronary embolism complicating aortic valve endocarditis: treatment with placement of an intracoronary stent. Clin Cardiol. 1997. 20:885–888.
Article10. Granger EK, Rankin J, Larbalestier RI, Hockings BE. Obstruction of the right coronary artery ostium by an aortic valve papillary fibroelastoma. Heart Lung Circ. 2005. 14:266–268.
Article11. Rigatelli G. Normal angiogram in patients with acute coronary syndrome: searching for unusual substrates of myocardial ischemia. Int J Cardiol. 2005. 99:25–27.
Article12. Alpert JS. Myocardial infarction with angiographically normal coronary arteries. Arch Intern Med. 1994. 154:265–269.
Article13. Proudfit WL, Bruschke VG, Sones FM Jr. Clinical course of patients with normal or slightly or moderately abnormal coronary arteriograms: 10-year follow-up of 521 patients. Circulation. 1980. 62:712–717.
Article14. Terefe YG, Niraj A, Pradhan J, Kondur A, Afonso L. Myocardial infarction with angiographically normal coronary arteries in the contemporary era. Coron Artery Dis. 2007. 18:621–626.
Article15. Bounhoure JP, Ouldzen H, Carrié D, Alibelli MJ, Puel J. Myocardial infarction with "angiographycally normal coronary arteries" myth or reality? Bull Acad Natl Med. 2007. 191:815–824.16. Raymond R, Lynch J, Underwood D, Leatherman J, Razavi M. Myocardial infarction and normal coronary arteriography: a 10 year clinical and risk analysis of 74 patients. J Am Coll Cardiol. 1988. 11:471–477.
Article17. Larsen AI, Galbraith PD, Ghali WA, Norris CM, Graham MM, Knudtson ML. APPROACH Investigators. Characteristics and outcomes of patients with acute myocardial infarction and angiographically normal coronary arteries. Am J Cardiol. 2005. 95:261–263.
Article18. Kang WY, Jeong MH, Ahn YK, Kim JH, Chae SC, Kim YJ, et al. Korea Acute Myocardial Infarction Registry Investigators. Are patients with angiographically near-normal coronary arteries who present as acute myocardial infarction actually safe? Int J Cardiol. 2011. 146:207–212.
Article19. Bugiardini R, Manfrini O, De Ferrari GM. Unanswered questions for management of acute coronary syndrome: risk stratification of patients with minimal disease or normal findings on coronary angiography. Arch Intern Med. 2006. 166:1391–1395.
Article20. French JK, White HD. Clinical implications of the new definition of myocardial infarction. Heart. 2004. 90:99–106.
Article21. Raymond R, Lynch J, Underwood D, Leatherman J, Razavi M. Myocardial infarction and normal coronary arteriography: a 10 year clinical and risk analysis of 74 patients. J Am Coll Cardiol. 1988. 11:471–477.
Article22. Fournier JA, Sánchez-González A, Quero J, Cortacero JA, Cabello A, Revello A, et al. Normal angiogram after myocardial infarction in young patients: a prospective clinical-angiographic and long-term follow-up study. Int J Cardiol. 1997. 60:281–287.23. Da Costa A, Isaaz K, Faure E, Mourot S, Cerisier A, Lamaud M. Clinical characteristics, aetiological factors and long-term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3-year follow-up study of 91 patients. Eur Heart J. 2001. 22:1459–1465.
Article24. Golzio PG, Orzan F, Ferrero P, Bobbio M, Bergerone S, Di Leo M, et al. Myocardial infarction with normal coronary arteries: ten-year follow-up. Ital Heart J. 2004. 5:732–738.25. Brecker SJ, Stevenson RN, Roberts R, Uthayakumar S, Timmis AD, Balcon R. Acute myocardial infarction in patients with normal coronary arteries. BMJ. 1993. 307:1255–1256.
Article26. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999. 340:115–126.27. Yun KH, Oh SK, Park EM, Kim HJ, Shin SH, Lee EM, et al. An increased monocyte count predicts coronary artery spasm in patients with resting chest pain and insignificant coronary artery stenosis. Korean J Intern Med. 2006. 21:97–102.
Article28. Bassuk SS, Rifai N, Ridker PM. High-sensitivity C-reactive protein: clinical importance. Curr Probl Cardiol. 2004. 29:439–493.29. Ammann P, Marschall S, Kraus M, Schmid L, Angehrn W, Krapf R, et al. Characteristics and prognosis of myocardial infarction in patients with normal coronary arteries. Chest. 2000. 117:333–338.
Article30. Richards AM, Nicholls MG, Yandle TG, Frampton C, Espiner EA, Turner JG, et al. Plasma N-terminal pro-brain natriuretic peptide and adrenomedullin: new neurohormonal predictors of left ventricular function and prognosis after myocardial infarction. Circulation. 1998. 97:1921–1929.
Article31. Nguyen TH, Neil CJ, Sverdlov AL, Mahadavan G, Chirkov YY, Kucia AM, et al. N-terminal pro-brain natriuretic protein levels in takotsubo cardiomyopathy. Am J Cardiol. 2011. 108:1316–1321.
Article32. Abdulla J, Asferg C, Kofoed KF. Prognostic value of absence or presence of coronary artery disease determined by 64-slice computed tomography coronary angiography a systematic review and meta-analysis. Int J Cardiovasc Imaging. 2011. 27:413–420.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Evaluation in Patients with Acute Myocardial Infarction with or without Significant Coronary Artery Stenosis
- Coronary-Pulmonary Fistulas Involving All Three Major Coronary Arteries Co-Existing With Myocardial Infarction
- Effect of Angina Pectoris before Acute Myocardial Infarction on Degree of Residual Stenosis after Successful Coronary Thrombolysis
- Correlation between Abnormal Q Wave in Leads I or aVL and First Diagonal Branch Stenosis in Patients with Acute Myocardial Infarction
- Acute Myocardial Infarction Occurring at a Preexisting Intermediate Coronary Artery Stenosis
