Treatment of Chronic Isolated Finger Flexor Tenosynovitis Through 50% Dehydrated Alcohol Installation
- Affiliations
-
- 1Department of Rehabilitation Medicine and Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Rehabilitation Medicine, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea. rekhs@nhimc.or.kr
- KMID: 2266618
- DOI: http://doi.org/10.5535/arm.2013.37.4.586
Abstract
- The isolated idiopathic finger flexor tenosynovitis is a rare condition, related to diversed etiologies. The traditional treatment of flexor tenosynovitis includes medications and injection of steroids. If the conservative treatment is not effective, surgical management is usually recommended. And alcohol installations have been rarely performed. We are reporting an extremely rare case of a 56-year-old man who had chronic idiopathic isolated finger flexor tenosynovitis which was treated through alcohol injections. The patient had not yet been treated despite of medication and serial injections of steroid. We performed 1 mL of 50% ethanol injection for the initial treatment and the second injection was done in the same way 10 months later due to the improvements of the patient's clinical symptoms and images of the follow-up ultrasonography. As a result, the authors suggest alcohol installation as an alternative non-surgical treatment for flexor tenosynovitis when other conservative managements are not effective enough.
Keyword
MeSH Terms
Figure
-
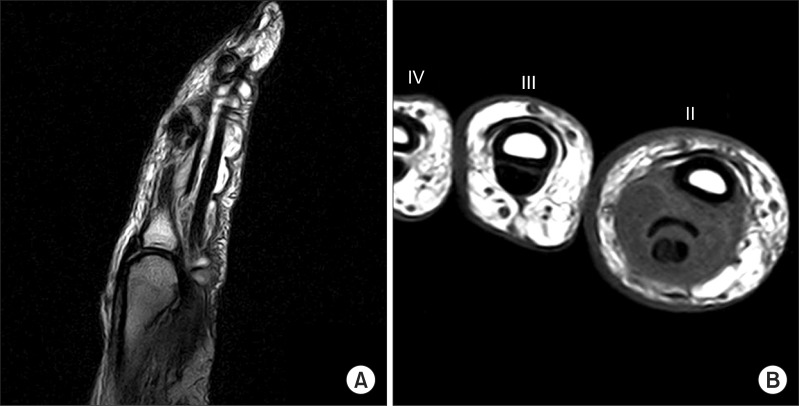
Fig. 1 Magnetic resonance images of right index finger. (A) Sagittal T2-weighted image showing accumulation of fluid around flexor tendon with lobulated margin and thickening of tendon, without definite abnormalities in the adjacent bones. (B) Note the reactive diffuse thickening of visceral layer of tendon sheath and synovial effusion in the right index finger (II) and the cross-sectional size of the index finger (II) is much larger relative to that of the middle finger (III).
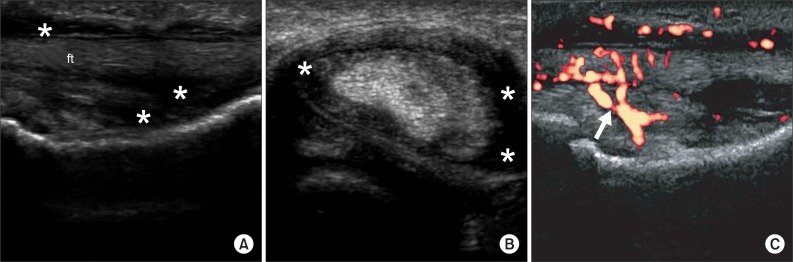
Fig. 2 Pretreatment ultrasonography images of chronic right index finger swelling. (A) Longitudinal image of the right index finger demonstrated a flexor tendon sheath distended by echogenic synovial fluid effusion (asterisks) surrounding the flexor tendon (ft). (B) Sagittal image of the right index finger showed synovial effusion (asterisks). (C) Power Doppler sonography image showed increased blood flow (arrow) within the synovial sheath.
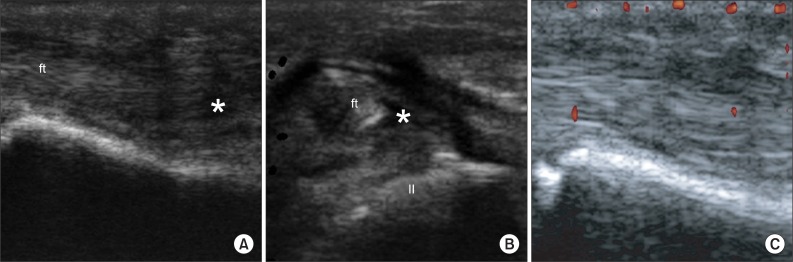
Fig. 3 Follow-up ultrasonography images of right index finger taken 22 months later after 1st injection. (A) Longitudinal images shows synovial fluid effusion (asterisk) of the right index finger is clearly decreased. (B) Sagittal images of the right index finger (II) shows synovial effusions are significantly reduced. (C) Power Doppler sonography image shows the disappearance of blood flow in synovial sheath, compared with previous findings.
Cited by 1 articles
-
Ultrasound-Guided 50% Ethyl Alcohol Injection for Patients With Malleolar and Olecranon Bursitis: A Prospective Pilot Study
Ji Seong Hong, Hyoung Seop Kim, Jin Hyung Lee
Ann Rehabil Med. 2016;40(2):310-317. doi: 10.5535/arm.2016.40.2.310.
Reference
-
1. Klug JD. MR diagnosis of tenosynovitis about the wrist. Magn Reson Imaging Clin N Am. 1995; 3:305–312. PMID: 7553024.
Article2. McGrath MH. Local steroid therapy in the hand. J Hand Surg Am. 1984; 9:915–921. PMID: 6392402.
Article3. Al-Qattan MM, Al-Namla A, Al-Thunayan A, Al-Omawi M. Tuberculosis of the hand. J Hand Surg Am. 2011; 36:1413–1421. PMID: 21764526.
Article4. Maffulli N, Longo UG, Loppini M, Denaro V. Current treatment options for tendinopathy. Expert Opin Pharmacother. 2010; 11:2177–2186. PMID: 20569088.
Article5. Rosenthal EA. Tenosynovitis: tendon and nerve entrapment. Hand Clin. 1987; 3:585–609. PMID: 3693421.
Article6. Jung JM, Kim JO, Yun YH, Koh YD, Yoo JD, Jung DH, et al. Tenosynovectomy for chronic flexor tenosynovitis at the wrist. J Korean Soc Surg Hand. 2004; 9:83–88.7. Bush DC, Schneider LH. Tuberculosis of the hand and wrist. J Hand Surg Am. 1984; 9:391–398. PMID: 6725899.
Article8. Bianchi S, Martinoli C. Ultrasound of the musculoskeletal system. Heidelberg: Springer;2007.9. Shin JB, Joo SH, Kim HS, Cho HK. Treatment of synovial proliferative subdeltoid bursitis through alcohol installation: a case report. J Korean Acad Rehabil Med. 2010; 34:106–109.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tuberculous Tenosynovitis of Flexor Tendon of the Hand
- Tuberculous Tenosynovitis and Ulnar Bursitis of the Wrist
- A Case of Trigger Finger Following Longitudinal Tear of Flexor Digitorum Superficialis after Repeated Closed Injury
- Tuberculous Tenosynovitis: A case report
- Solitary Synovial Chondromatosis as a Cause of Trigger Finger at the A3 Pulley: A Case Report
