Ann Rehabil Med.
2014 Oct;38(5):702-706. 10.5535/arm.2014.38.5.702.
Locked-in Syndrome due to Central Pontine Myelinolysis: Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Chungnam National University School of Medicine, Daejeon, Korea. shapil21@cnuh.co.kr
- KMID: 2266507
- DOI: http://doi.org/10.5535/arm.2014.38.5.702
Abstract
- Central pontine myelinolysis (CPM) classically occurs in alcoholics, malnourished individuals, chronic liver diseases, and rapid correction of hyponatremia. This report presents locked-in syndrome due to CPM following rapid correction of hyponatremia. A 44-year-old male came to the hospital due to a short period of loss of consciousness. He was alert and had no focal neurological abnormalities at admission. The serum sodium concentration was 118 mEq/L and was corrected to 134 mEq/L in the first 18 hours. One week later, progressive weakness in limbs developed and he progressed to a complete quadriplegic state and bulbar palsy, with only eye blinking preserved. Brain magnetic resonance imaging revealed a characteristic hyperintense signal abnormality in both pons, so he was diagnosed to locked-in syndrome caused by CPM. The patient gradually improved following continuous intensive rehabilitation for more than 2 years. He was able to move all joint muscles against gravity in generally and he could gait under supervision.
MeSH Terms
Figure
-
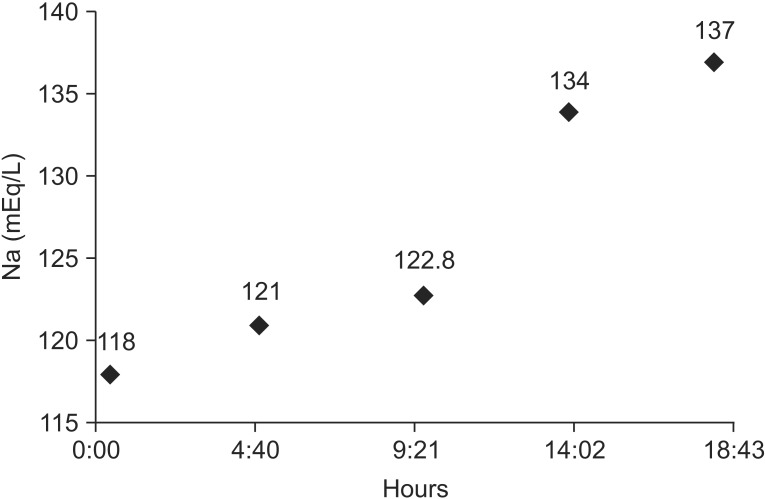
Fig. 1 Changes in serum sodium (Na) concentrations during the first day.
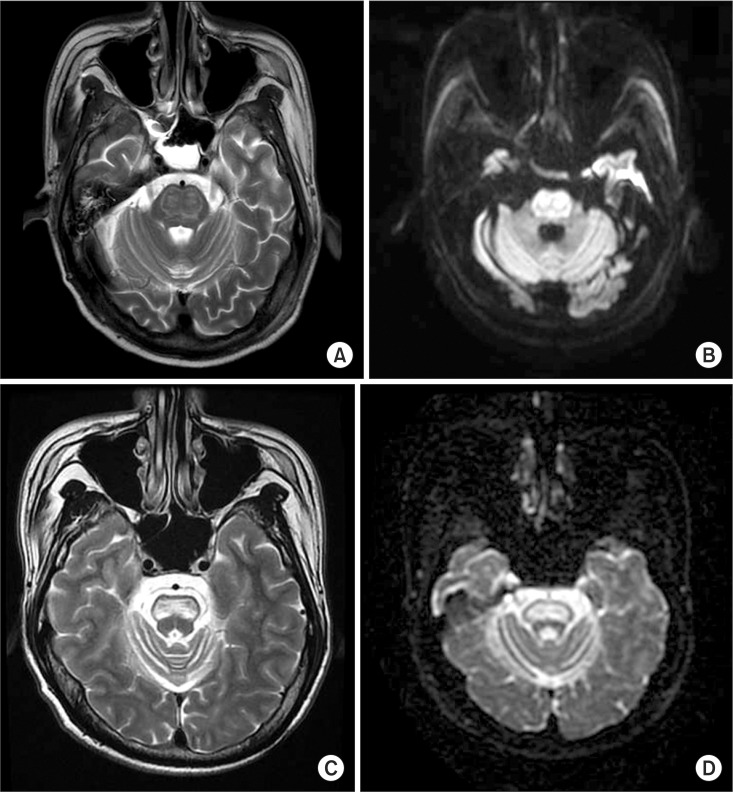
Fig. 2 (A, B) Brain MRI shows T2- and diffusion-weighted imaging high signal intensity lesion in the bilateral pons, osmotic demyelination syndrome in pons 10 days after onset of symptoms. (C, D) Encephalomalacia at the site of initial high signal intensity lesion in pons after 1 year.
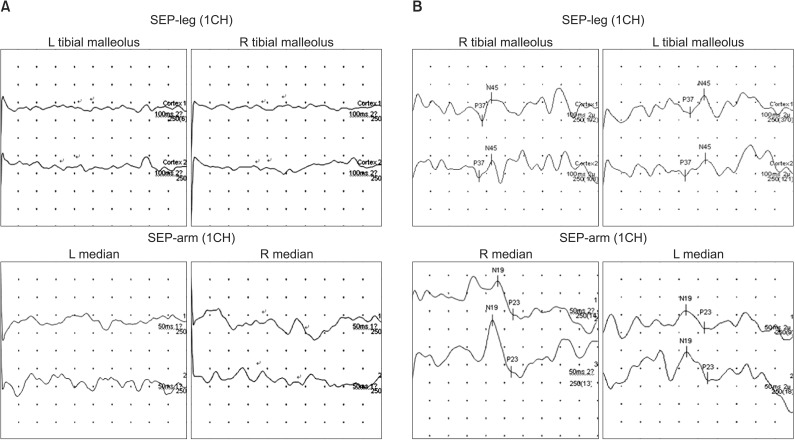
Fig. 3 (A) Somatosensory evoked potential (SEP) study stimulating both tibial nerves and median nerves shows absent potentials, bilaterally at first admission. (B) SEP study stimulating the tibial nerve shows prolonged latency of P37, N45 potentials, bilaterally and SEP study stimulating both median nerves shows prolonged latency of N19, P23 potentials at 3 years after onset.
Reference
-
1. Adams RD, Victor M, Mancall EL. Central pontine myelinolysis. AMA Arch Neurol Psychiatry. 1959; 81:154–172.
Article2. Newell KL, Kleinschmidt-DeMasters BK. Central pontine myelinolysis at autopsy; a twelve year retrospective analysis. J Neurol Sci. 1996; 142:134–139. PMID: 8902733.
Article3. Lampl C, Yazdi K. Central pontine myelinolysis. Eur Neurol. 2002; 47:3–10. PMID: 11803185.
Article4. Casanova E, Lazzari RE, Lotta S, Mazzucchi A. Locked-in syndrome: improvement in the prognosis after an early intensive multidisciplinary rehabilitation. Arch Phys Med Rehabil. 2003; 84:862–867. PMID: 12808539.5. Huang WY, Weng WC, Peng TI, Ro LS, Yang CW, Chen KH. Central pontine and extrapontine myelinolysis after rapid correction of hyponatremia by hemodialysis in a uremic patient. Ren Fail. 2007; 29:635–638. PMID: 17654329.
Article6. Kwon HG, Jang SH. Motor recovery mechanism in a quadriplegic patient with locked-in syndrome. NeuroRehabilitation. 2012; 30:113–117. PMID: 22430576.
Article7. Sterns RH, Riggs JE, Schochet SS Jr. Osmotic demyelination syndrome following correction of hyponatremia. N Engl J Med. 1986; 314:1535–1542. PMID: 3713747.
Article8. Kallakatta RN, Radhakrishnan A, Fayaz RK, Unnikrishnan JP, Kesavadas C, Sarma SP. Clinical and functional outcome and factors predicting prognosis in osmotic demyelination syndrome (central pontine and/or extrapontine myelinolysis) in 25 patients. J Neurol Neurosurg Psychiatry. 2011; 82:326–331. PMID: 20826870.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of central pontine and extrapontine myelinolysis with early hypermetabolism on 18FDG-PET scan
- Central Pontine Myelinolysis Presenting With Cerebellar Ataxia
- Central Pontine and Extrapontine Myelinolysis in a Patient with Traumatic Brain Injury Following Not Rapid Correction of Hyponatremia: A Case Report
- A Case of Subacute Onset Choreoathetosis as Sequelae of Central Pontine and Extrapontine Myelinolysis
- Central Pontine Myelinolysis Induced by Alcohol Withdrawal: A Case Report
