Ann Pediatr Endocrinol Metab.
2013 Dec;18(4):214-217. 10.6065/apem.2013.18.4.214.
Nongoitrous autoimmune thyroiditis with facial palsy
- Affiliations
-
- 1Department of Pediatrics, Catholic University of Daegu School of Medicine, Daegu, Korea. kimjk@cu.ac.kr
- KMID: 2266358
- DOI: http://doi.org/10.6065/apem.2013.18.4.214
Abstract
- We report a case of severe hypothyroidism with nongoitrous, autoimmune thyroiditis and pituitary hyperplasia in a 13-year-old boy, who presented with sudden palsy on the left side of his face. Prednisolone and antiviral medication was administered. However, the facial palsy did not improve completely. The medications were replaced with thyroxine, and the facial palsy recovered. Endocrinological testing showed severe hypothyroidism as follows: thyroid stimulating hormone (TSH) level >100 microIU/mL, T4 of 1.04 microg/dL, T3 of 0.31 ng/mL, and free T4 of 0.07 ng/dL. Level of serum antithyroid peroxidase antibodies was 1,933.39 IU/mL, and that of antithyroglobulin antibodies was 848.16 IU/mL. Level of TSH receptor antibodies was >40 IU/L. Bioassay result for TSH receptor stimulating antibodies was negative. Thyroid sonography revealed no increase in the size or vascularity of the bilateral gland. Thyroid scintigraphy with 99mTc showed decreased uptake, and magnetic resonance imaging demonstrated an enlarged pituitary gland.
Keyword
MeSH Terms
-
Adolescent
Antibodies
Biological Assay
Facial Paralysis*
Humans
Hyperplasia
Hypothyroidism
Magnetic Resonance Imaging
Male
Paralysis
Peroxidase
Pituitary Gland
Prednisolone
Radionuclide Imaging
Receptors, Thyrotropin
Thyroid Gland
Thyroiditis, Autoimmune*
Thyrotropin
Thyroxine
Antibodies
Peroxidase
Prednisolone
Receptors, Thyrotropin
Thyrotropin
Thyroxine
Figure
-
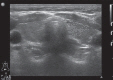
Fig. 1 Thyroid sonography shows a heterogenous internal structure without an increase in size or vascularity of the bilateral gland.

Fig. 2 Thyroid scintigraphy with 99mTc shows a substantial decrease in uptake in both lobes.

Fig. 3 Magnetic resonance imaging demonstrates an enlarged pituitary gland, with upward convexity, 13.0 mm in height and 8 mm at the transverse diameter.
Reference
-
1. Yilmaz U, Cubukçu D, Yilmaz TS, Akinci G, Ozcan M, Guzel O. Peripheral facial palsy in children. J Child Neurol. 2013; 10. 04. [Epub]. http://dx.doi.org/10.1177/0883073813503990.
Article2. Earll JM, Kolb FO. Facial paralysis occurring with hypothyroidism: a report of two cases. Calif Med. 1967; 106:56–58. PMID: 6036455.3. Cox NH, Chew D, Williams JG, Morris AI. Bell's palsy associated with hypothyroidism. Br J Clin Pract. 1985; 39:158–159. PMID: 4015946.
Article4. Carle A, Pedersen IB, Knudsen N, Perrild H, Ovesen L, Jorgensen T, et al. Thyroid volume in hypothyroidism due to autoimmune disease follows a unimodal distribution: evidence against primary thyroid atrophy and autoimmune thyroiditis being distinct diseases. J Clin Endocrinol Metab. 2009; 94:833–839. PMID: 19088156.
Article5. Smith BR, Sanders J, Furmaniak J. TSH receptor antibodies. Thyroid. 2007; 17:923–938. PMID: 17900238.
Article6. Konishi J, Iida Y, Endo K, Misaki T, Nohara Y, Matsuura N, et al. Inhibition of thyrotropin-induced adenosine 3'5'-monophosphate increase by immunoglobulins from patients with primary myxedema. J Clin Endocrinol Metab. 1983; 57:544–549. PMID: 6135705.
Article7. Konishi J, Iida Y, Kasagi K, Misaki T, Nakashima T, Endo K, et al. Primary myxedema with thyrotrophin-binding inhibitor immunoglobulins: clinical and laboratory findings in 15 patients. Ann Intern Med. 1985; 103:26–31. PMID: 2860835.8. Arikawa K, Ichikawa Y, Yoshida T, Shinozawa T, Homma M, Momotani N, et al. Blocking type antithyrotropin receptor antibody in patients with nongoitrous hypothyroidism: its incidence and characteristics of action. J Clin Endocrinol Metab. 1985; 60:953–959. PMID: 2858492.9. Chiovato L, Vitti P, Santini F, Lopez G, Mammoli C, Bassi P, et al. Incidence of antibodies blocking thyrotropin effect in vitro in patients with euthyroid or hypothyroid autoimmune thyroiditis. J Clin Endocrinol Metab. 1990; 71:40–45. PMID: 2164529.10. Takasu N, Yamada T, Takasu M, Komiya I, Nagasawa Y, Asawa T, et al. Disappearance of thyrotropin-blocking antibodies and spontaneous recovery from hypothyroidism in autoimmune thyroiditis. N Engl J Med. 1992; 326:513–518. PMID: 1732791.11. Brown RS, Bellisario RL, Botero D, Fournier L, Abrams CA, Cowger ML, et al. Incidence of transient congenital hypothyroidism due to maternal thyrotropin receptor-blocking antibodies in over one million babies. J Clin Endocrinol Metab. 1996; 81:1147–1151. PMID: 8772590.
Article12. Takasu N, Yamashiro K, Ochi Y, Sato Y, Nagata A, Komiya I, et al. TSBAb (TSH-stimulation blocking antibody) and TSAb (thyroid stimulating antibody) in TSBAb-positive patients with hypothyroidism and Graves' patients with hyperthyroidism. Horm Metab Res. 2001; 33:232–237. PMID: 11383928.13. Takasu N, Matsushita M. Changes of TSH-Stimulation blocking antibody (TSBAb) and thyroid stimulating antibody (TSAb) over 10 years in 34 TSBAb-positive patients with hypothyroidism and in 98 TSAb-positive Graves' patients with hyperthyroidism: reevaluation of TSBAb and TSAb in TSH-receptor-antibody (TRAb)-positive patients. J Thyroid Res. 2012; 2012:182176. PMID: 22655217.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histopathologic study of the so called 'palpation thyroiditis'
- Pathophysiology of Chronic Autoimmune Thyroiditis
- Association Kikuchi disease with Hashimoto thyroiditis: a case report and literature review
- A case of Kikuchi-Fujimoto disease with autoimmune thyroiditis
- A Case of Bilateral Bell's Palsy with Uncontrolled Diabetes Mellitus
