J Rheum Dis.
2015 Apr;22(2):123-126. 10.4078/jrd.2015.22.2.123.
Idiopathic Retroperitoneal Fibrosis Associated with Rheumatoid Arthritis in a Patient with Concomitant Chronic B Viral Hepatitis
- Affiliations
-
- 1Department of Rheumatology, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea. rheuma@yonsei.ac.kr
- 2Department of Internal Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 3Department of Haemato-Oncology, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2222916
- DOI: http://doi.org/10.4078/jrd.2015.22.2.123
Abstract
- Retroperitoneal fibrosis (RPF) is a rare, progressive disease characterized by chronic non specific inflammation of the retroperitoneum. Although the pathogenesis of idiopathic retroperitoneal fibrosis (IRF) remains unclear, IRF has been reported in association with autoimmune disorders. However, few cases of IRF associated with rheumatoid arthritis (RA) have been reported. We experienced a rare case of IRF in a patient with RA and chronic B viral hepatitis. A 39-year-old Korean man with RA and hepatitis B was referred to our hospital due to left hydronephrosis. An abdominal computed tomography (CT) scan and magnetic resonance imaging (MRI) showed a diffuse infiltrating retroperitoneal mass around the abdominal aorta and left ureter. The patient underwent intraureteral stent insertion and was treated with corticosteroid. Three months later, the follow up abdominal CT showed that the retroperitoneal mass had decreased in size. Herein, we report the first case of coexistent IRF, RA, and chronic B viral hepatitis with a literature review.
MeSH Terms
Figure
-
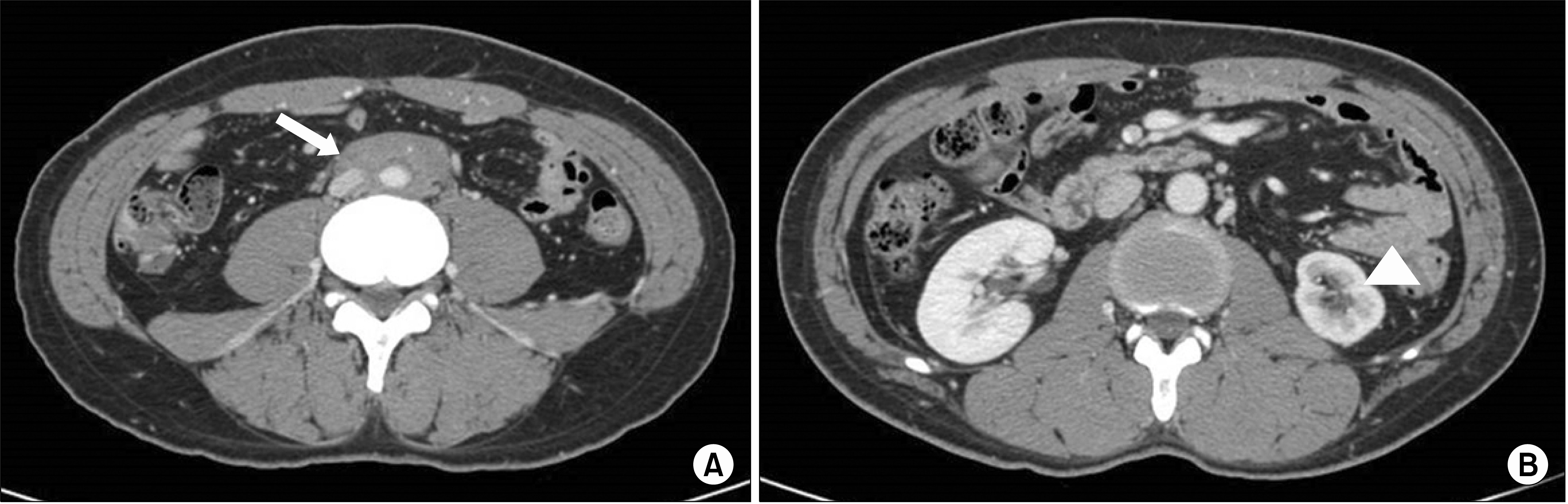
Figure 1. (A) Abdominal computed tomography shows a diffuse infiltrating soft tissue mass (about 5.0×2.5×10.3 cm sized) extending from the lower abdominal aorta to the level of the iliac bifurcation and left ureteral obstruction (arrow). (B) Atrophic change on left kidney (arrowhead).

Figure 2. (A) The lesion reveals a fibrous proliferation with broad anatomizing bands of collagen. Occasionally lymphoid aggregates are noted (arrow) (H&E, ×40). (B) Fibrous proliferation with sclerotic collagen bands (H&E, ×200).

Figure 3. The retroperitoneal mass was decreased at the follow-up abdominal computed tomography (arrow).
Reference
-
1. Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet. 2006; 367:241–51.
Article2. Pipitone N, Vaglio A, Salvarani C. Retroperitoneal fibrosis. Best Pract Res Clin Rheumatol. 2012; 26:439–48.
Article3. Vaglio A, Corradi D, Manenti L, Ferretti S, Garini G, Buzio C. Evidence of autoimmunity in chronic periaortitis: a prospective study. Am J Med. 2003; 114:454–62.
Article4. Miller OF, Smith LJ, Ferrara EX, McAleer IM, Kaplan GW. Presentation of idiopathic retroperitoneal fibrosis in the pediatric population. J Pediatr Surg. 2003; 38:1685–8.
Article5. Tsai TC, Chang PY, Chen BF, Huang FY, Shih SL. Retroperitoneal fibrosis and juvenile rheumatoid arthritis. Pediatr Nephrol. 1996; 10:208–9.
Article6. Couderc M, Mathieu S, Dubost JJ, Soubrier M. Retroperitoneal fibrosis during etanercept therapy for rheumatoid arthritis. J Rheumatol. 2013; 40:1931–3.
Article7. Vaglio A, Palmisano A, Ferretti S, Alberici F, Casazza I, Salvarani C, et al. Peripheral inflammatory arthritis in patients with chronic periaortitis: report of five cases and review of the literature. Rheumatology (Oxford). 2008; 47:315–8.
Article8. Corradi D, Maestri R, Palmisano A, Bosio S, Greco P, Manenti L, et al. Idiopathic retroperitoneal fibrosis: clinicopathologic features and differential diagnosis. Kidney Int. 2007; 72:742–53.
Article9. Martorana D, Vaglio A, Greco P, Zanetti A, Moroni G, Salvarani C, et al. Chronic periaortitis and HLA-DRB1*03: another clue to an autoimmune origin. Arthritis Rheum. 2006; 55:126–30.
Article10. Rodríguez-Hernández MJ, Viciana P, Cordero E, López-Cortés LF, Pachón J. Retroperitoneal fibrosis in a patient with human immunodeficiency virus infection. Arch Intern Med. 1998; 158:301–2.11. Hofbauer LC, Magerstadt RA, Heufelder AE. Hepatitis C related cryoglobulinemia associated with retroperitoneal fibrosis. J Rheumatol. 1996; 23:554–7.12. Pelkmans LG, Aarnoudse AJ, Hendriksz TR, van Bommel EF. Value of acutephase reactants in monitoring disease activity and treatment response in idiopathic retroperitoneal fibrosis. Nephrol Dial Transplant. 2012; 27:2819–25.
Article13. Vaglio A, Versari A, Fraternali A, Ferrozzi F, Salvarani C, Buzio C. (18)F-fluorodeoxyglucose positron emission tomography in the diagnosis and followup of idiopathic retroperitoneal fibrosis. Arthritis Rheum. 2005; 53:122–5.
Article14. Li KP, Zhu J, Zhang JL, Huang F. Idiopathic retroperitoneal fibrosis (RPF): clinical features of 61 cases and literature review. Clin Rheumatol. 2011; 30:601–5.
Article15. Kim TW, Kim MN, Kwon JW, Kim KM, Kim SH, Kim W, et al. Risk of hepatitis B virus reactivation in patients with asthma or chronic obstructive pulmonary disease treated with corticosteroids. Respirology. 2010; 15:1092–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Development of Liver Cirrhosis in a Elderly Healthy Hepatitis B Carrier with Rheumatoid Arthritis Treated with Low-dose Methotrexate (MTX)
- Systemic Lupus Erythematosus Presenting with Idiopathic Retroperitoneal Fibrosis
- Idiopathic Retroperitoneal Fibrosis: Report of a Case
- A Case of Chronic Active Hepatitis Developed in Patient with Psoriasis after Long-term Methotrexate Treatment
- A Case of Polyarthritis Associated with Reactivation of Chronic Hepatitis B Virus Infection
