The Morphological Changes in Main Corneal Incision (2.2 mm vs. 2.8 mm) Evaluated Using Anterior Segment Optical Coherence Tomography
- Affiliations
-
- 1The Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. shadik@yuhs.ac
- KMID: 2217263
- DOI: http://doi.org/10.3341/jkos.2013.54.6.877
Abstract
- PURPOSE
To investigate wound characteristics and ultrastructural changes in the 2.2-mm and 2.8-mm main corneal incisions.
METHODS
Forty-four eyes of 34 patients undergoing cataract surgery were randomized to receive a 2.2-mm or 2.8-mm main corneal incision. All incisions were evaluated 1, 7, and 30 days postoperatively using anterior segment optical coherence tomography. The angle, length, maximal thickness of the incision, and if present, corneal gap length and incision gap area were calculated. The existence of Descemet's membrane detachment was recorded.
RESULTS
The mean endothelial gap length and gap area of the 2.2-mm wound were larger than the 2.8-mm, with the only statistically significant difference observed on postoperative day 30 (p = 0.015 and 0.027, respectively). There was no difference in the mean incision angle, length, and corneal thickness between the 2 incision sizes. The ratio of Descemet's membrane detachment increased with older age and low postoperative IOP, but not associated with incision size (p < 0.05).
CONCLUSIONS
Both the 2.2-mm and 2.8-mm main corneal incisions showed excellent wound healing outcome without significant postoperative complications. Older patients with low postoperative IOP required a more careful wound care management. The incision parameters in the present study can be used as an indicator of the healing process to reduce wound-related complications.
Keyword
MeSH Terms
Figure
-
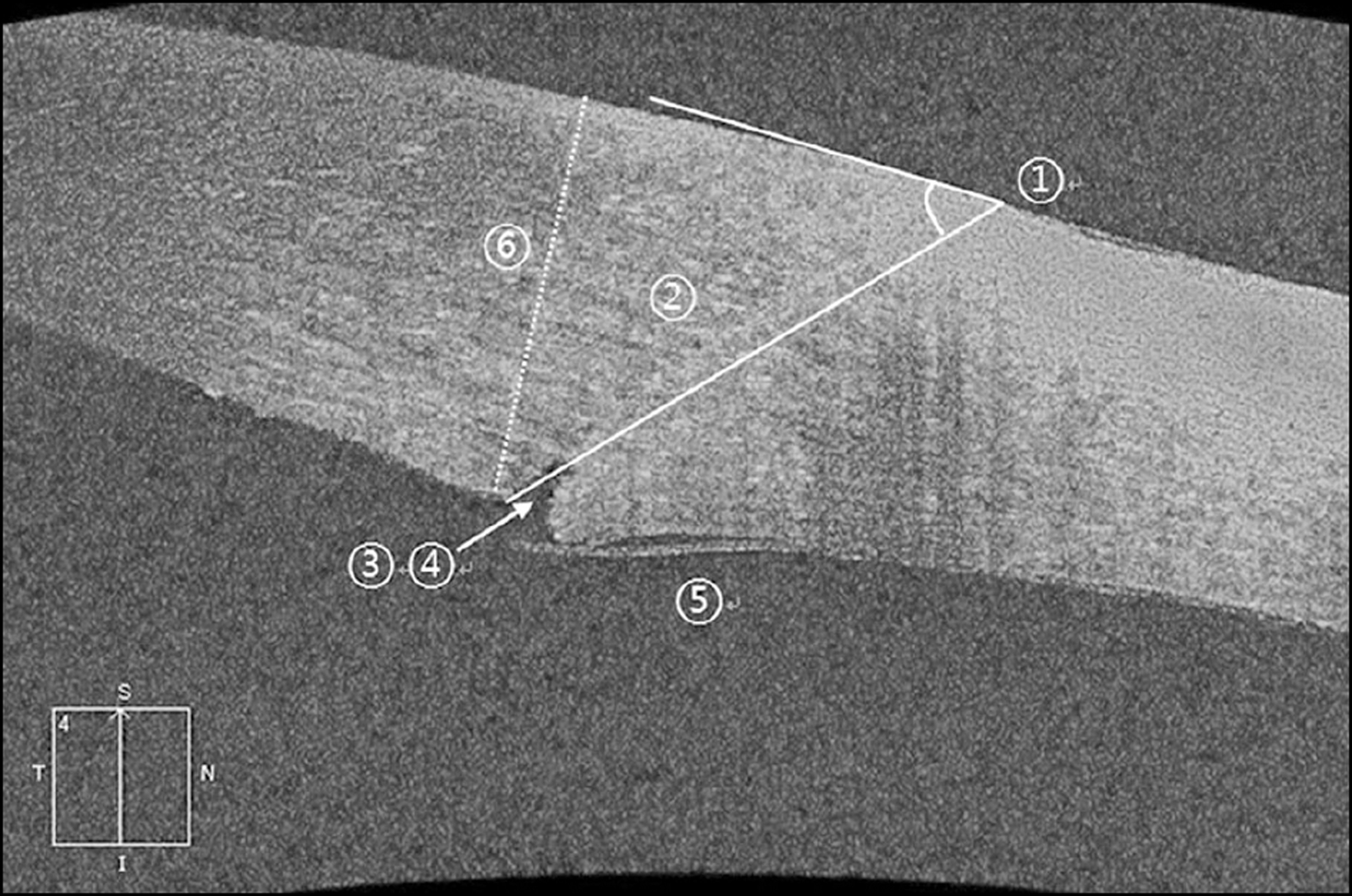
Figure 1. Anterior segment OCT (optical coherence tomography) image showing a clear corneal incision site postoperatively. The definition of incision site parameters: 1) Incision angle (The angle between the line that joins the epithelial and endo-thelial ends of the incision and the tangential line on the cor-neal surface) 2) Incision length (The total length of the main incision measured from the wound entry to its exit point) 3) Epithelial/endothelial gap length (The length that lines inside of the gap, the longer one is selected, if present) 4) Epithelial/ endothelial gap area (The area inside of the gap, if present) 5) Descemet’s membrane detachment 6) Maximal corneal thick-ness at the incision site.

Figure 2. Results of AS-OCT parameter, (A) Mean angle (°); (B) Mean length (μ m); (C) Mean corneal thickness at incision site (μ m); (D) Mean endothelial gap length (μ m); (E) Mean endothelial gap area (μ m2) (* p < 0.05).
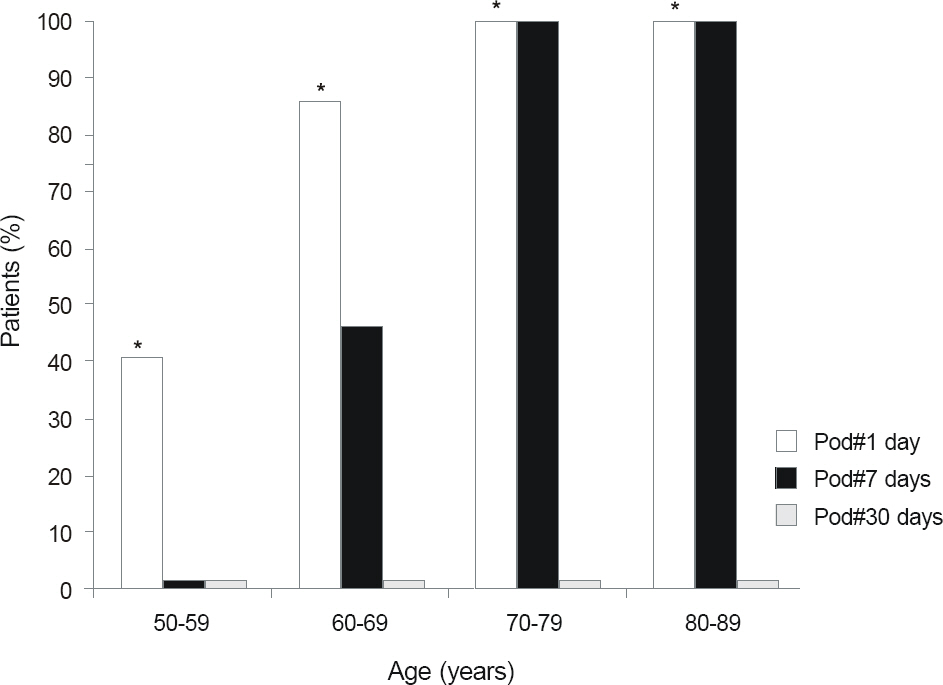
Figure 3. The ratio of postoperative Descemet’s membrane detachment by age (* p < 0.05).
Cited by 1 articles
-
The Effectiveness of Topical Chemotherapy for the Primary Treatment of Ocular Surface Squamous Neoplasia
Im Gyu Kim, Sung Yu, Gwang Ja Lee, Kyoo Won Lee, Young Jeung Park
J Korean Ophthalmol Soc. 2017;58(2):147-155. doi: 10.3341/jkos.2017.58.2.147.
Reference
-
References
1. Kelman CD. Phaco-emulsification and aspiration. A new techni-que of cataract removal. A preliminary report. Am J Ophthalmol. 1967; 64:23–35.
Article2. Crema AS, Walsh A, Yamane Y, Nosé W. Comparative study of coaxial phacoemulsification and microincision cataract surgery. One-year follow-up. J Cataract Refract Surg. 2007; 33:1014–8.
Article3. Ku HC, Kim HJ, Joo CK. The comparison of astigmatism according to the incision size in small incision cataract surgery. J Korean Ophthalmol Soc. 2005; 46:416–21.4. Jee DH, Lee PY, Joo CK. The comparison of astigmatism according to the incision size in cataract operation. J Korean Ophthalmol Soc. 2003; 44:594–8.5. Nagaki Y, Hayasaka S, Kadoi C. . Bacterial endophthalmitis after small-incision cataract surgery: effect of incision placement and intraocular lens type. J Cataract Refract Surg. 2003; 29:20–6.6. Eifrig CW, Flynn HW Jr, Scott IU, Newton J. Acute-onset post-operative endophthalmitis: review of incidence and visual out-comes (1995-2001). Ophthalmic Surg Lasers. 2002; 33:373–8.
Article7. Taban M, Behrens A, Newcomb RL. . Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol. 2005; 123:613–20.8. Miller JJ, Scott IU, Flynn HW Jr. . Acute-onset endoph-thalmitis after cataract surgery (2000-2004): incidence, clinical settings, and visual acuity outcomes after treatment. Am J Ophthalmol. 2005; 139:983–7.
Article9. Monica ML, Long DA. Nine-year safety with self-sealing corneal tunnel incision in clear cornea cataract surgery. Ophthalmology. 2005; 112:985–6.
Article10. Masket S. Is there a relationship between clear corneal cataract in-cisions and endophthalmitis? J Cataract Refract Surg. 2005; 31:643–5.
Article11. Wallin T, Parker J, Jin Y. . Cohort study of 27 cases of endoph-thalmitis at a single institution. J Cataract Refract Surg. 2005; 31:735–41.
Article12. Choi JA, Chung SK, Kim HS. Comparative study of microcoaxial cataract surgery and conventional cataract surgery. J Korean Ophthalmol Soc. 2008; 49:904–10.
Article13. Taban M, Rao B, Reznik J. . Dynamic morphology of suture-less cataract wounds–effect of incision angle and location. Surv Ophthalmol. 2004; 49:Suppl 2. S62–72.
Article14. Torres LF, Saez-Espinola F, Colina JM. . In vivo architectural analysis of 3.2 mm clear corneal incisions for phacoemulsification using optical coherence tomography. J Cataract Refract Surg. 2006; 32:1820–6.
Article15. Fine IH, Hoffman RS, Packer M. Profile of clear corneal cataract incisions demonstrated by ocular coherence tomography. J Cataract Refract Surg. 2007; 33:94–7.
Article16. Vasavada V, Vasavada V, Raj SM, Vasavada AR. Intraoperative performance and postoperative outcomes of microcoaxial phaco- emulsification. Observational study. J Cataract Refract Surg. 2007; 33:1019–24.17. Osher RH, Injev VP. Microcoaxial phacoemulsification: Part 1: laboratory studies. J Cataract Refract Surg. 2007; 33:401–7.18. Cavallini GM, Pupino A, Masini C. . Bimanual micro-phacoemulsification and Acri. Smart intraocular lens implantation combined with vitreoretinal surgery. J Cataract Refract Surg. 2007; 33:1253–8.19. Schallhorn JM, Tang M, Li Y. . Optical coherence tomography of clear corneal incisions for cataract surgery. J Cataract Refract Surg. 2008; 34:1561–5.
Article20. Dupont-Monod S, Labbé A, Fayol N. . In vivo architectural analysis of clear corneal incisions using anterior segment optical coherence tomography. J Cataract Refract Surg. 2009; 35:444–50.
Article21. Calladine D, Tanner V. Optical coherence tomography of the ef-fects of stromal hydration on clear corneal incision architecture. J Cataract Refract Surg. 2009; 35:1367–71.
Article22. Elkady B, Piñero D, Alió JL. Corneal incision quality: Microincision cataract surgery versus microcoaxial phacoemulsification. J Cataract Refract Surg. 2009; 35:466–74.
Article23. McGowan BL. Mechanism for development of endophthalmitis. J Cataract Refract Surg. 1994; 20:111.
Article24. Can I, Bayhan HA, Celik H, Bostancı Ceran B. Anterior segment optical coherence tomography evaluation and comparison of main clear corneal incisions in microcoaxial and biaxial cataract surgery. J Cataract Refract Surg. 2011; 37:490–500.
Article25. Can I, Takmaz T, Genç I. Half-moon supracapsular nucleofractis phacoemulsification: Safety, efficacy, and functionality. J Cataract Refract Surg. 2008; 34:1958–65.
Article26. Xia Y, Liu X, Luo L. . Early changes in clear cornea incision af-ter phacoemulsification: an anterior segment optical coherence to-mography study. Acta Ophthalmol. 2009; 87:764–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Structural Analysis of Different Incision Sizes and Stromal Hydration in Cataract Surgery Using Anterior Segment Optical Coherence Tomography
- Comparison of Anterior Segment Parameters Obtained by Anterior Segment Optical Coherence Tomography and Dual Rotating Scheimpflug Camera
- Changes in Anterior Chamber Depth and Angle After Phacoemulsification measured by Anterior Segment Optical Coherence Tomography
- Features of Pinguecula Analyzed by Anteroir Segment Optical Coherence Tomography
- Changes in Corneal Thickness in Congenital Glaucoma, Using Anterior Segment Optical Coherence Tomography
