Korean J Ophthalmol.
2015 Feb;29(1):23-30. 10.3341/kjo.2015.29.1.23.
Structural Analysis of Different Incision Sizes and Stromal Hydration in Cataract Surgery Using Anterior Segment Optical Coherence Tomography
- Affiliations
-
- 1Department of Ophthalmology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. eyedr0823@hotmail.com
- KMID: 2360134
- DOI: http://doi.org/10.3341/kjo.2015.29.1.23
Abstract
- PURPOSE
To analyze healing changes of corneal wounds of different corneal incision sizes with or without stromal hydration in cataract surgery using anterior segment optical coherence tomography.
METHODS
Cataract surgeries were performed by a single surgeon and 2.2- and 2.8-mm corneal incisions were made using a diamond blade (ME-759; Meyco, Biel-Bienne, Swiss). Patients were divided into four groups according to incision size (2.2 and 2.8 mm), and with/without stromal hydration. Fifteen eyes were assigned to each group and incision wounds were measured using anterior segment optical coherence tomography at 2 hours, 1 day, 1 week, 1 month, and 3 months postoperatively. Corneal thickness, incision length and incision angle were measured and existence of epithelial, endothelial gaping and Descemet's membrane detachment was evaluated.
RESULTS
Incision thickness was greater in the group with stromal hydration than in the group without on operation day (p < 0.05). Stromal hydration exerted greater influence in the 2.2-mm incision group than in the 2.8-mm incision group. Corneal thickness decreased more rapidly in the stromal hydration group than in the group with no hydration (p = 0.022). Endothelial gaping was greater in the 2.2-mm incision group than in the 2.8-mm incision group 1 day, 1 month, and 3 months after surgery (p = 0.035, p = 0.009, and p = 0.008, respectively). No other statistical significance was observed between the two groups (2.2 and 2.8 mm) during follow-up regarding corneal thickness, epithelial gaping and Descemet's membrane detachment.
CONCLUSIONS
Corneal wounds with a smaller incision could be more vulnerable to external stimuli such as stromal hydration and are less stable than those with a larger incision.
MeSH Terms
Figure
-
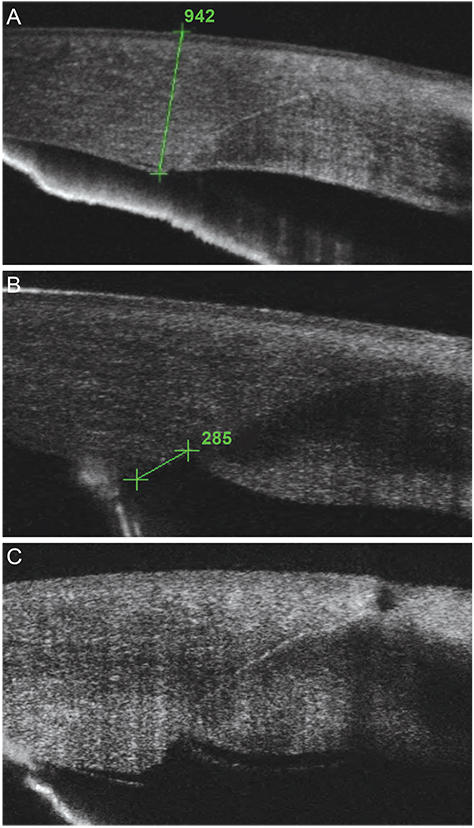
Fig. 1 (A) Thickness of corneal incision, (B) endothelial gape, and (C) Descemet's membrane detachment.
Reference
-
1. Li YJ, Kim HJ, Joo CK. Early changes in corneal edema following torsional phacoemulsification using anterior segment optical coherence tomography and Scheimpflug photography. Jpn J Ophthalmol. 2011; 55:196–204.2. Jun B, Berdahl JP, Kuo AN, et al. Corneal wound architecture and integrity after torsional and mixed phacoemulsification: evaluation of standard and microincisional coaxial techniques. Ophthalmic Surg Lasers Imaging. 2010; 41:128–134.3. Fukuda S, Kawana K, Yasuno Y, Oshika T. Wound architecture of clear corneal incision with or without stromal hydration observed with 3-dimensional optical coherence tomography. Am J Ophthalmol. 2011; 151:413–419.4. Can I, Bayhan HA, Celik H, Bostancı Ceran B. Anterior segment optical coherence tomography evaluation and comparison of main clear corneal incisions in microcoaxial and biaxial cataract surgery. J Cataract Refract Surg. 2011; 37:490–500.5. Cavallini GM, Campi L, Torlai G, et al. Clear corneal incisions in bimanual microincision cataract surgery: long-term wound-healing architecture. J Cataract Refract Surg. 2012; 38:1743–1748.6. Calladine D, Tanner V. Optical coherence tomography of the effects of stromal hydration on clear corneal incision architecture. J Cataract Refract Surg. 2009; 35:1367–1371.7. Wang L, Dixit L, Weikert MP, et al. Healing changes in clear corneal cataract incisions evaluated using Fourier-domain optical coherence tomography. J Cataract Refract Surg. 2012; 38:660–665.8. Torres LF, Saez-Espinola F, Colina JM, et al. In vivo architectural analysis of 3.2 mm clear corneal incisions for phacoemulsification using optical coherence tomography. J Cataract Refract Surg. 2006; 32:1820–1826.9. Fine IH, Hoffman RS, Packer M. Profile of clear corneal cataract incisions demonstrated by ocular coherence tomography. J Cataract Refract Surg. 2007; 33:94–97.10. Dupont-Monod S, Labbe A, Fayol N, et al. In vivo architectural analysis of clear corneal incisions using anterior segment optical coherence tomography. J Cataract Refract Surg. 2009; 35:444–450.11. Mifflin MD, Kinard K, Neuffer MC. Comparison of stromal hydration techniques for clear corneal cataract incisions: conventional hydration versus anterior stromal pocket hydration. J Cataract Refract Surg. 2012; 38:933–937.12. Mackool RJ, Russell RS. Strength of clear corneal incisions in cadaver eyes. J Cataract Refract Surg. 1996; 22:721–725.13. Taban M, Rao B, Reznik J, et al. Dynamic morphology of sutureless cataract wounds: effect of incision angle and location. Surv Ophthalmol. 2004; 49:Suppl 2. S62–S72.14. Herretes S, Stark WJ, Pirouzmanesh A, et al. Inflow of ocular surface fluid into the anterior chamber after phacoemulsification through sutureless corneal cataract wounds. Am J Ophthalmol. 2005; 140:737–740.15. Masket S. Is there a relationship between clear corneal cataract incisions and endophthalmitis. J Cataract Refract Surg. 2005; 31:643–645.16. Osher RH, Injev VP. Thermal study of bare tips with various system parameters and incision sizes. J Cataract Refract Surg. 2006; 32:867–872.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Morphological Changes in Main Corneal Incision (2.2 mm vs. 2.8 mm) Evaluated Using Anterior Segment Optical Coherence Tomography
- Changes in Anterior Chamber Depth and Angle After Phacoemulsification measured by Anterior Segment Optical Coherence Tomography
- Changes of Anterior Chamber Depth and Angle After Cataract Surgery Measured by Anterior Segment OCT
- Changes in Anterior Chamber Configuration after Cataract Surgery as Measured by Anterior Segment Optical Coherence Tomography
- Utility of the Anterior Segment Optical Coherence Tomography for Measurements of Central Corneal Thickness
