The Short-Term Effect of Limbal Relaxing Incision and Compression Suture on Post-Penetrating Keratoplasty Astigmatism
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. kmk9@snu.ac.kr
- 2Department of Laboratory of Corneal Regenerative Medicine and Ocular Immunology, Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- KMID: 2214995
- DOI: http://doi.org/10.3341/jkos.2011.52.10.1142
Abstract
- PURPOSE
To investigate the short-term effect of limbal relaxing incisions accompanied by compression sutures on postoperative astigmatism in penetrating keratoplasty.
METHODS
The medical records of patients who underwent penetrating keratoplasty, were followed-up for at least 18 months and had residual astigmatism greater than 4.0 diopters (D), were retrospectively analyzed. The patients had paired limbal relaxing incisions on the steep axis and compression sutures on the flat axis. The paired limbal relaxing incision was done for 2 clock hours each with a depth of 85% of the corneal thickness, and the compression sutures with an average of 3.2 bites were added with a Troutman operating keratometer guide. The visual acuities, corneal astigmatism and complications were evaluated at 1 month and 6 months.
RESULTS
At 1 month after the surgery, the best corrected visual acuities (log MAR) improved from 0.840 to 0.674 (p = 0.037) except for 1 patient with immediate postoperative rejection and another patient with a pre-existing cataract. The mean corneal astigmatism was reduced from 9.118 +/- 3.158 D to 4.982 +/- 3.063 D (p = 0.021). At 6 months after the surgery, the mean corneal astigmatism increased to 5.489 +/- 2.670 D (p = 0.008), and the effect of surgery became statistically insignificant (p = 0.477).
CONCLUSIONS
Paired limbal relaxing incisions and compression sutures were effective short-term on reducing residual corneal astigmatism and improving visual acuities in keratoplasty patients with high astigmatism, but became less effective on corneal astigmatism at 6 months.
MeSH Terms
Figure
-
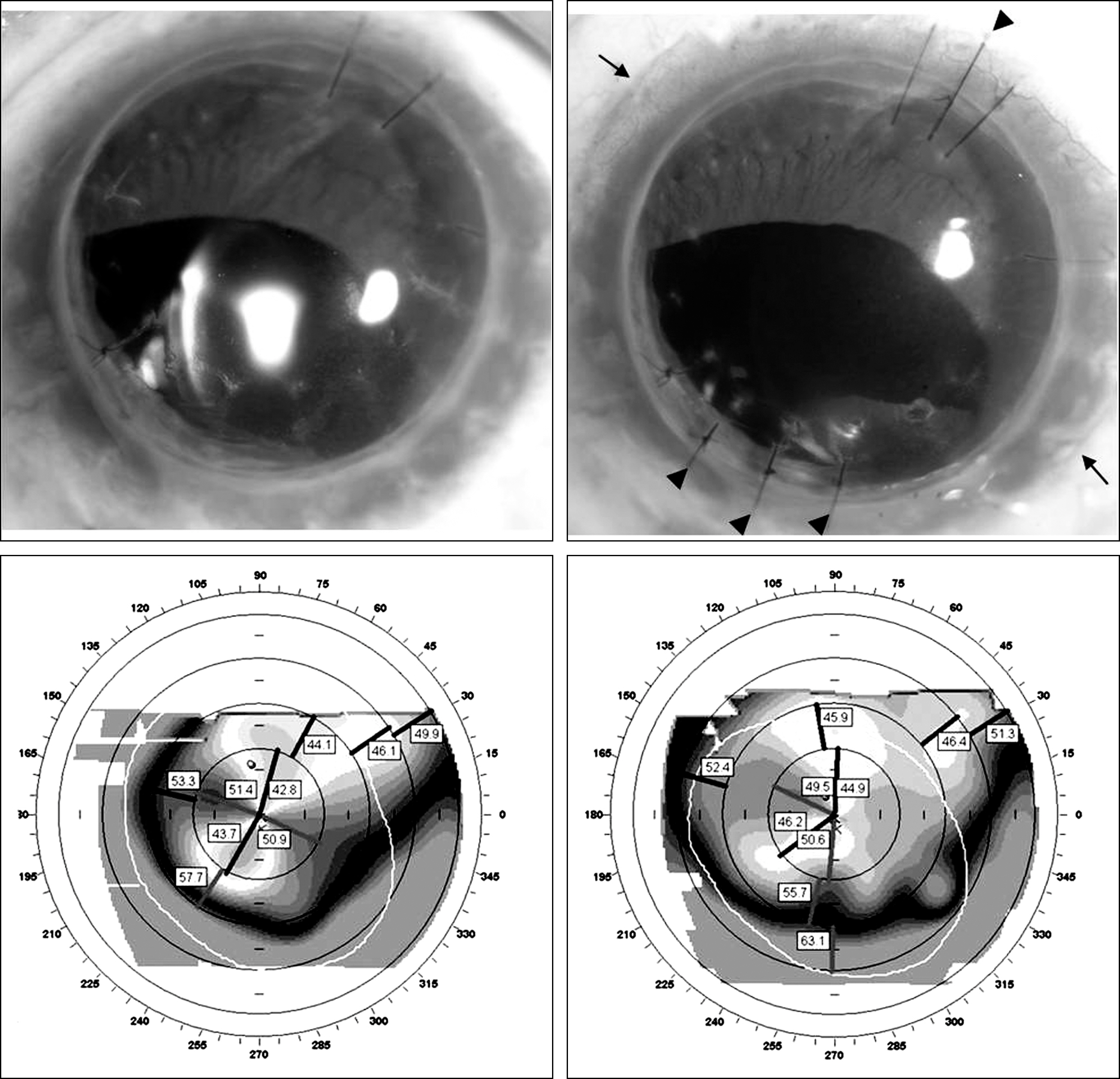
Figure 1. Preoperative and postoperative photographs and topographs. These figures show typical topographic changes after limbal relaxing incision and compression sutures. The figures on the left are preoperative photographs and topographs with a simulated keratometry of 7.6 diopters. Paired relaxing incisions (arrows) were done at the steep axis on the limbus, and 4 compression sutures (arrow heads) were added at the flat axis on the junction between graft and host. The figures on the right are postoperative photographs and topographs with a simulated keratometry of 2.3 diopters.
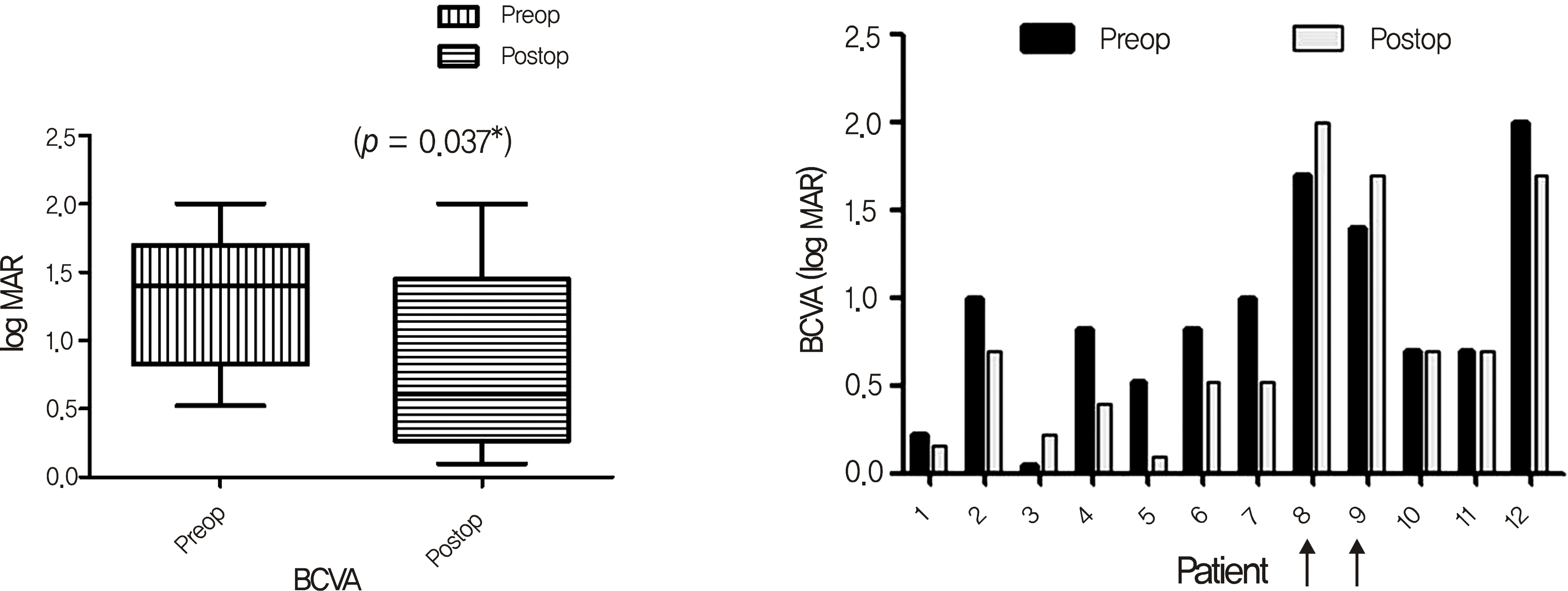
Figure 2. Improvement in BCVA after limbal relaxing incision and compression sutures. Best corrected visual acuities (BCVA, log MAR) improved from 0.840 to 0.674, and got worse in cases of rejection (patient 8, arrow) and cataract progression (patient 9, arrow).
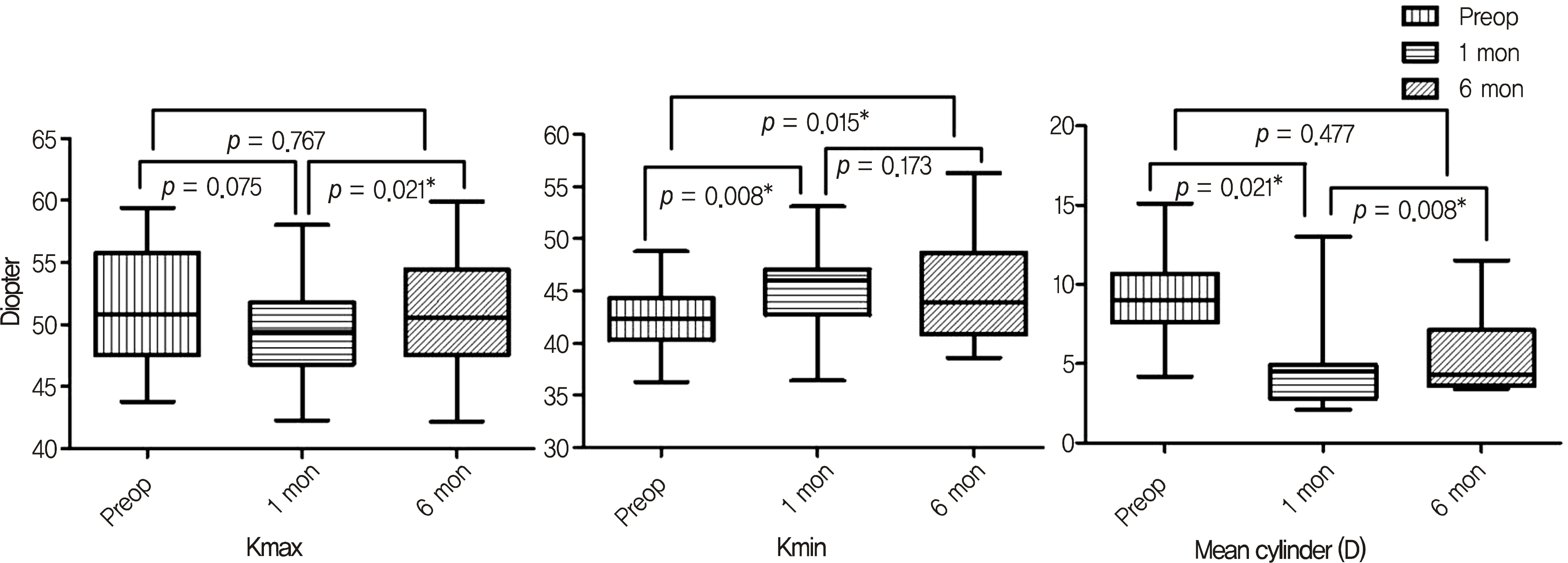
Figure 3. Mean topographic changes in Kmax, Kmin and topographic astigmatism. At 1 month after the surgery, mean corneal power of steep axis (Kmax) was reduced from 51.3 ± 4.8 D to 49.8 ± 4.1 D (p = 0.075) and mean corneal power of flat axis (Kmin) increased from 42.1 ± 3.1 D to 44.2 ± 5.2 D (p = 0.008). As a result mean corneal astigmatism was reduced from 9.118 ± 3.158 D to 4.982 ± 3.063 D (p = 0.021). At 6 months after the surgery, mean corneal astigmatism increased to 5.489 ± 2.670 D (p = 0.008), and the effect of surgery became statistically insignificant (p = 0.477).
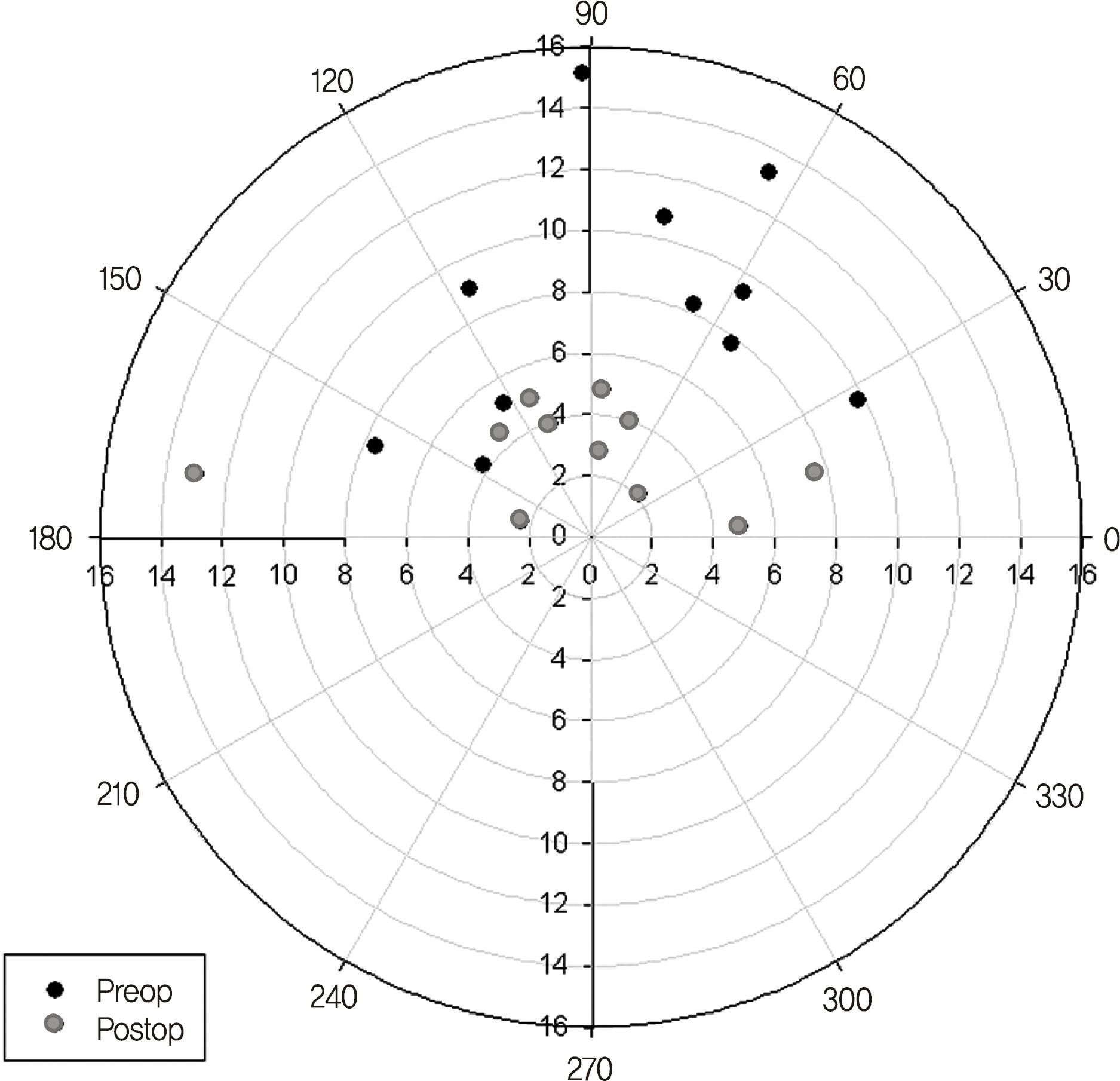
Figure 4. Vector analysis of mean topographic astigmatism. This polar plot demonstrates the magnitude and the axis of mean topographic astigmatism. Each concentric ring represents 2.0 diopters of change. Vector analysis of mean topographic astigmatism shows changes of 7.9 ± 5.4 diopters. Gray dots (postoperative astigmatism) are closer to the center compared with black dots (preoperative astigmatism).
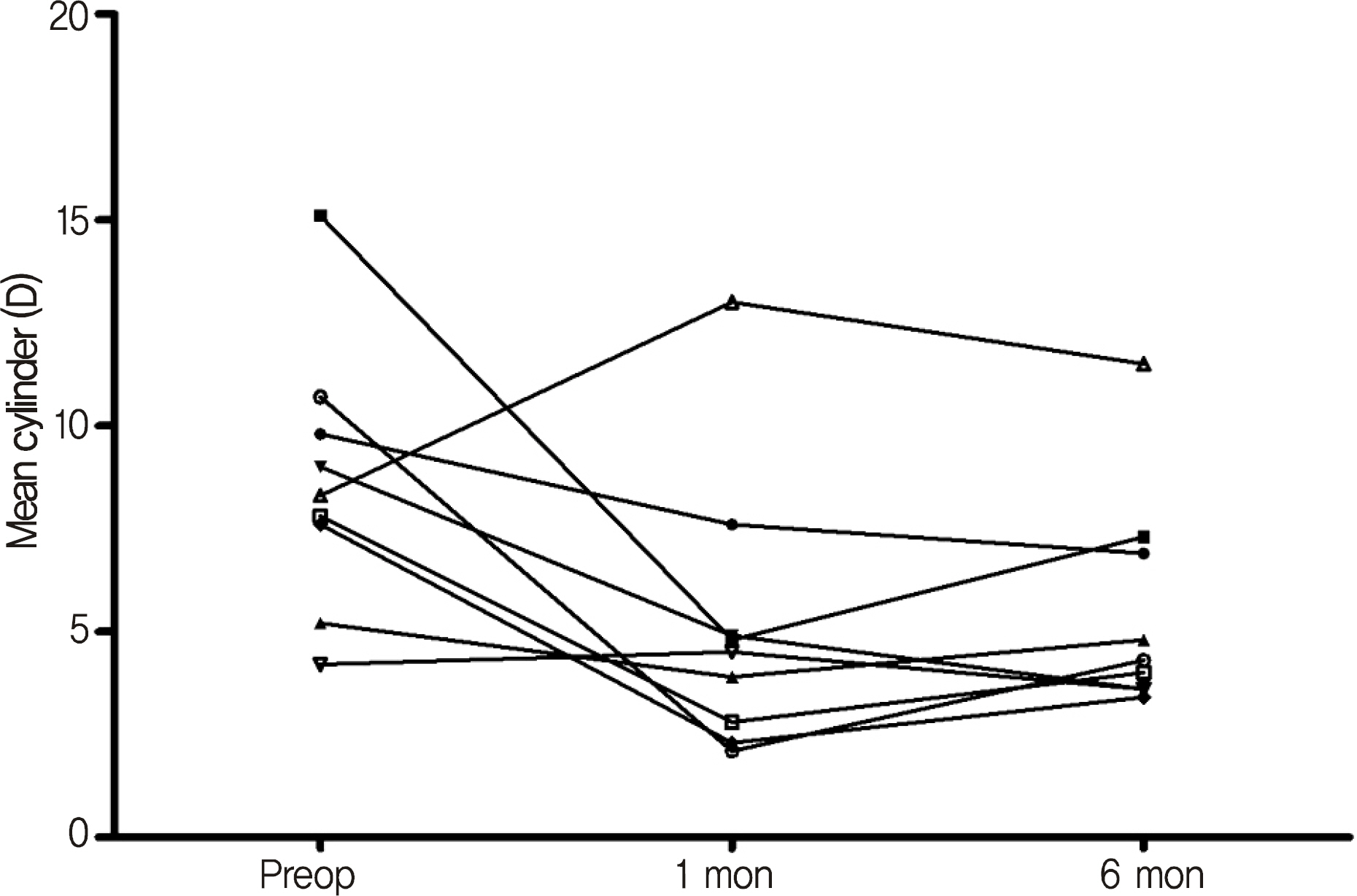
Figure 5. Further follow up of corneal astigmatism. Mean topographic astigmatism increases in some patients after the short-term effect of limbal relaxing incision and compression sutures.
Cited by 3 articles
-
Clinical Outcomes of Beveled, Full Thickness Astigmatic Keratotomy
Bu Ki Kim, Su Joung Mun, Dae Gyu Lee, Young Taek Chung
J Korean Ophthalmol Soc. 2015;56(8):1160-1169. doi: 10.3341/jkos.2015.56.8.1160.Clinical Outcomes of Combined Procedure of Astigmatic Keratotomy and Laser in situ Keratomileusis
Bu Ki Kim, Su Joung Mun, Dae Gyu Lee, Young Taek Chung
J Korean Ophthalmol Soc. 2016;57(3):353-360. doi: 10.3341/jkos.2016.57.3.353.Short-term Clinical Outcomes of Implantable Collamer Lens Implantation with Simultaneous Full Thickness Astigmatic Keratotomy
Buki Kim, Sujoung Mun, Hyuntae Choi, Youngtaek Chung
J Korean Ophthalmol Soc. 2017;58(8):916-923. doi: 10.3341/jkos.2017.58.8.916.
Reference
-
References
1. Murta JN, Amaro L, Tavares C, Mira JB. Astigmatism after penetrating keratoplasty. Role of the suture technique. Doc Ophthalmol. 1994; 87:331–6.2. Williams KA, Roder D, Esterman A, et al. Factors predictive of corneal graft survival. Report from the Australian Corneal Graft Registry. Ophthalmology. 1992; 99:403–14.3. Busin M, Monks T, al-Nawaiseh I. Different suturing techniques variously affect the regularity of postkeratoplasty astigmatism. Ophthalmology. 1998; 105:1200–5.
Article4. Eggink FA, Nuijts RM. A new technique for rigid gas permeable contact lens fitting following penetrating keratoplasty. Acta Ophthalmol Scand. 2001; 79:245–50.
Article5. Kuryan J, Channa P. Refractive surgery after corneal transplant. Curr Opin Ophthalmol. 2010; 21:259–64.
Article6. Wilkins MR, Mehta JS, Larkin DF. Standardized arcuate keratotomy for postkeratoplasty astigmatism. J Cataract Refract Surg. 2005; 31:297–301.
Article7. Koay PY, McGhee CN, Crawford GJ. Effect of a standard paired arcuate incision and augmentation sutures on postkeratoplasty astigmatism. J Cataract Refract Surg. 2000; 26:553–61.
Article8. Javadi MA, Feizi S, Yazdani S, et al. Outcomes of augmented relaxing incisions for postpenetrating keratoplasty astigmatism in keratoconus. Cornea. 2009; 28:280–4.
Article9. Claesson M, Armitage WJ. Astigmatism and the impact of relaxing incisions after penetrating keratoplasty. J Refract Surg. 2007; 23:284–9.
Article10. Bochmann F, Schipper I. Correction of postkeratoplasty astigmatism with keratotomies in the host cornea. J Cataract Refract Surg. 2006; 32:923–8.
Article11. Alessio G, Boscia F, La Tegola MG, Sborgia C. Corneal interactive programmed topographic ablation customized photorefractive keratectomy for correction of postkeratoplasty astigmatism. Ophthalmology. 2001; 108:2029–37.
Article12. Lazzaro DR, Haight DH, Belmont SC, et al. Excimer laser keratectomy for astigmatism occurring after penetrating keratoplasty. Ophthalmology. 1996; 103:458–64.13. Kwitko S, Marinho DR, Rymer S, Ramos Filho S. Laser in situ keratomileusis after penetrating keratoplasty. J Cataract Refract Surg. 2001; 27:374–9.
Article14. Webber SK, Lawless MA, Sutton GL, Rogers CM. LASIK for post penetrating keratoplasty astigmatism and myopia. Br J Ophthalmol. 1999; 83:1013–8.
Article15. Lee HS, Kim MS. Factors related to the correction of astigmatism by LASIK after penetrating keratoplasty. J Refract Surg. 2010; 26:960–5.
Article16. Kaye SB, Campbell SH, Davey K, Patterson A. A method for assessing the accuracy of surgical technique in the correction of astigmatism. Br J Ophthalmol. 1992; 76:738–40.
Article17. Chang DH, Hardten DR. Refractive surgery after corneal transplantation. Curr Opin Ophthalmol. 2005; 16:251–5.
Article18. Nubile M, Carpineto P, Lanzini M, et al. Femtosecond laser arcuate keratotomy for the correction of high astigmatism after keratoplasty. Ophthalmology. 2009; 116:1083–92.
Article19. Vajpayee RB, Sharma N, Sinha R, et al. Laser in-situ keratomileusis after penetrating keratoplasty. Surv Ophthalmol. 2003; 48:503–14.
Article20. Nassaralla BR, Nassaralla JJ. Laser in situ keratomileusis after penetrating keratoplasty. J Refract Surg. 2000; 16:431–7.
Article21. Ranchod TM, McLeod SD. Wound dehiscence in a patient with keratoconus after penetrating keratoplasty and LASIK. Arch Ophthalmol. 2004; 122:920–1.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Astigmatism after Penetrating Keratoplasty According to Suture Methods
- Suture Tension Adjustment of Single Running Suture in Penetrating Keratoplasty
- The Effect of Different Suturing Techniques on Astigmatism after Penetrating Keratoplasty
- Changes in Astigmatism after Suture Removal in Penetrating Keratoplasty
- Effects of Adjustment of a Continuous Suture on Astigmatic Correction after Penetrating Keratoplasty
