The Effect of Different Suturing Techniques on Astigmatism after Penetrating Keratoplasty
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Hospital, Seoul, Korea. kmk9@snu.ac.kr
- 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 1107527
- DOI: http://doi.org/10.3346/jkms.2008.23.6.1015
Abstract
- The purpose of this study was to compare the effects on astigmatism after penetrating keratoplasty with three different suture techniques. In this prospective study, 38 eyes of 38 patients underwent penetrating keratoplasty with three suturing techniques: interrupted, single running, and double running. Topographic astigmatism was measured at 2, 6, 12, and 18 months after keratoplasty. During 18 months after surgery, the interrupted suture group had higher astigmatism than the double running suture group. There was no significant difference in the amounts of astigmatism during the first year after keratoplasty between the single running and the double running suture group. However, at 18 months after surgery, when all sutures were out, the double running suture group (3.60+/-1.58 diopters) showed significantly less astigmatism than the single running group (5.65+/-1.61 diopters). In conclusion, post-keratoplasty astigmatism was the least in the double running suture group of the three suturing techniques at 18 months after penetrating keratoplasty.
Keyword
MeSH Terms
Figure
-
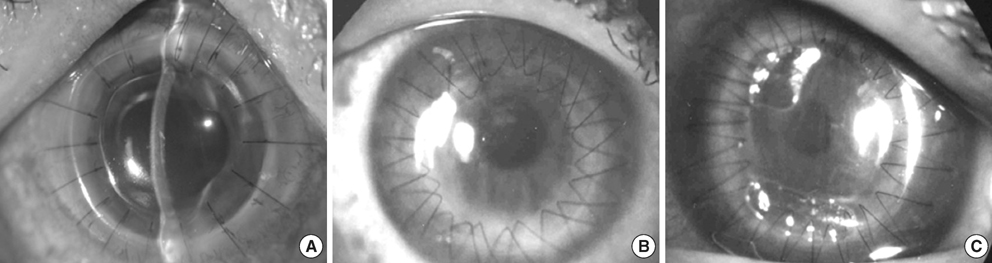
Fig. 1 Three suturing techniques in penetrating keratoplasty; interrupted (A), double running (B), and single running (C).
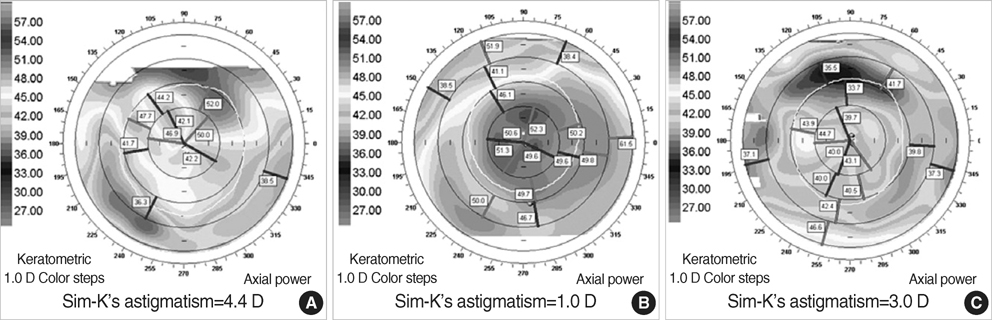
Fig. 2 Topographic astigmatism of representative cases with three different suture techniques by the Orbscan topographic system (A: interrupted suture, B: double running suture, C: single running suture). All three were done 12 to 18 months after surgery, when all the sutures were removed.
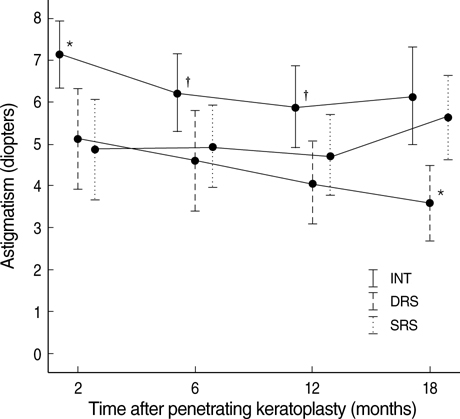
Fig. 3 The changes in astigmatism measured with the Orbscan (Orbtek Inc. Salt Lake City, UT, U.S.A.) at 2, 6, 12, and 18 months after penetrating keratoplasty in three groups. INT, DRS, and SRS represent interrupted suture, double running, and single running suture, respectively. Horizontal bars represent two standard errors of mean (SEM). *, Significantly different (p<0.05, Mann-Whitney U test) compared to other two groups, respectively; †, significantly different (p<0.05, Mann-Whitney U test) between INT and DRS groups.
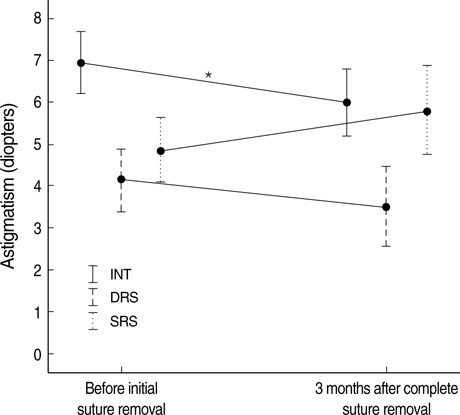
Fig. 4 Topographic astigmatism (Diopters, mean±SD) before initial suture removal and three months after suture removal in each suturing technique groups. INT, DRS, and SRS represent interrupted suture, double running, and single running suture, respectively. Horizontal bars represent two standard errors of mean (SEM). *, Significantly different astigmatism between before initial suture removal and three months after suture removal (p<0.05, Wilcoxon matched pairs signed ranks test).
Reference
-
1. Swinger CA. Postoperative astigmatism. Surv Ophthalmol. 1987. 31:219–248.
Article2. Serdarevic ON, Renard GJ, Pouliquen Y. Randomized clinical trial comparing astigmatism and visual rehabilitation after penetrating keratoplasty with and without intraoperative suture adjustment. Ophthalmology. 1994. 101:990–999.
Article3. Hoppenreijs VP, Van Rij G, Beekhuis WH, Rijneveld WJ, Rinkelvan Driel E. Causes of high astigmatism after penetrating keratoplasty. Doc Ophthalmol. 1993. 85:21–34.
Article4. Murta JN, Amaro L, Tavares C, Mira JB. Astigmatism after penetrating keratoplasty. Role of the suture technique. Doc Ophthalmol. 1994. 87:331–336.5. Seitz B, Langenbucher A, Kuchle M, Naumann GO. Impact of graft diameter on corneal power and the regularity of postkeratoplasty astigmatism before and after suture removal. Ophthalmology. 2003. 110:2162–2167.
Article6. Filatov V, Steinert RF, Talamo JH. Postkeratoplasty astigmatism with single running suture or interrupted sutures. Am J Ophthalmol. 1993. 115:715–721.
Article7. Boruchoff SA, Jensen AD, Dohlman CH. Comparison of suturing techniques in keratoplasty for keratoconus. Ann Ophthalmol. 1975. 7:433–436.8. Van Meter WS, Gussler JR, Soloman KD, Wood TO. Postkeratoplasty astigmatism control. Single continuous suture adjustment versus selective interrupted suture removal. Ophthalmology. 1991. 98:177–183.9. Frost NA, Wu J, Lai TF, Coster DJ. A review of randomized controlled trials of penetrating keratoplasty techniques. Ophthalmology. 2006. 113:942–949.
Article10. Ramirez M, Hodge DO, Bourne WM. Keratometric results during the first year after keratoplasty: adjustable single running suture technique versus double running suture technique. Ophthalmic Surg Lasers. 2001. 32:370–374.
Article11. Solano JM, Hodge DO, Bourne WM. Keratometric astigmatism after suture removal in penetrating keratoplasty: double running versus single running suture techniques. Cornea. 2003. 22:716–720.12. Spadea L, Cifariello F, Bianco G, Balestrazzi E. Long-term results of penetrating keratoplasty using a single or double running suture technique. Graefes Arch Clin Exp Ophthalmol. 2002. 240:415–419.
Article13. Mader TH, Yuan R, Lynn MJ, Stulting RD, Wilson LA, Waring GO 3rd. Changes in keratometric astigmatism after suture removal more than one year after penetrating keratoplasty. Ophthalmology. 1993. 100:119–126.
Article14. Hoffmann F. Suture technique for perforating keratoplasty. Klin Monatsbl Augenheilkd. 1976. 169:584–590.15. Binder PS. Selective suture removal can reduce postkeratoplasty astigmatism. Ophthalmology. 1985. 92:1412–1416.
Article16. McNeill JI, Aaen VJ. Long-term results of single continuous suture adjustment to reduce penetrating keratoplasty astigmatism. Cornea. 1999. 18:19–24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Astigmatism after Penetrating Keratoplasty According to Suture Methods
- Comparison of Corneal Astigmatism after Keratolasty with 3 Kinds of Suture Techniques
- Changes in Astigmatism after Suture Removal in Penetrating Keratoplasty
- Suture Tension Adjustment of Single Running Suture in Penetrating Keratoplasty
- Effects of Adjustment of a Continuous Suture on Astigmatic Correction after Penetrating Keratoplasty
