Detection of Intra-Abdominal Tumor Recurrence in Patients with Cholangiocarcinoma: Comparison of Contrast-Enhanced MDCT and 18F FDG-PET/CT
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hwasun Hospital, Chonnam National University, Medical School, Korea. yjeong@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Hospital, Chonnam National University, Medical School, Korea.
- 3Department of Surgery, Chonnam National University Hwasun Hospital, Chonnam National University, Medical School, Korea.
- 4Department of Nuclear Medicine, Chonnam National Hwasun University Hospital, Chonnam National University, Medical School, Korea.
- KMID: 2208955
- DOI: http://doi.org/10.3348/jksr.2010.62.2.149
Abstract
-
PURPOSE: This study was designed to compare the diagnostic accuracy between the use of contrast-enhanced CT (CECT) and PET/CT for the detection of tumor recurrence in post-operative patients with cholangiocarcinoma during follow-up.
MATERIALS AND METHODS
Twenty-five patients who had undergone abdominal CT and PET/CT examinations had clinical or imaging feature suspicious of recurrence. Ultimately, 16 patients (mean age, 65.1 years) were included in the study. The presence of recurrence was confirmed based on follow-up imaging (n = 10) or a biopsy (n = 6). Sensitivity, specificity and accuracy between the use of CECT and PET/CT were compared.
RESULTS
Sixteen patients were found to have tumor recurrence. On a per patient basis, the sensitivity, specificity and accuracy for the use of CECT for tumor recurrence were 69%, 50% and 65%, respectively. The sensitivity, specificity and accuracy for the use of PET/CT for tumor recurrence were 100%, 75% and 95%, respectively. On a per lesion basis, the sensitivity, specificity and accuracy for the use of CECT for tumor recurrence were 73%, 50% and 70%, respectively. The sensitivity, specificity and accuracy for the use of PET/CT for tumor recurrence were 100%, 75% and 97%, respectively. PET/CT had significantly higher sensitivity and accuracy as compared to CT for the detection on a per lesion basis for recurred cholangiocarcinoma (p < 0.01).
CONCLUSION
PET/CT was more sensitive and accurate for the detection of recurrence of cholangiocarcinoma as compared to CECT. A PET/CT examination should be included in post-operative follow-up studies for the evaluation of recurred cholangiocarcinoma.
MeSH Terms
Figure
-

Fig. 1 Local recurrence in a 57-year-old man who had a history of right hepatectomy, bile duct resection and hepaticojejunostomy for Klatskin tumor. A. Contrast-enhanced CT (CECT) reveals recurred mass (arrows) in the right side of peripancreatic area. Axial (B) and coronal (C) PET/CT show that focal hypermetabolic lesion (arrows) corresponds to a recurred mass (arrows) on CECT.
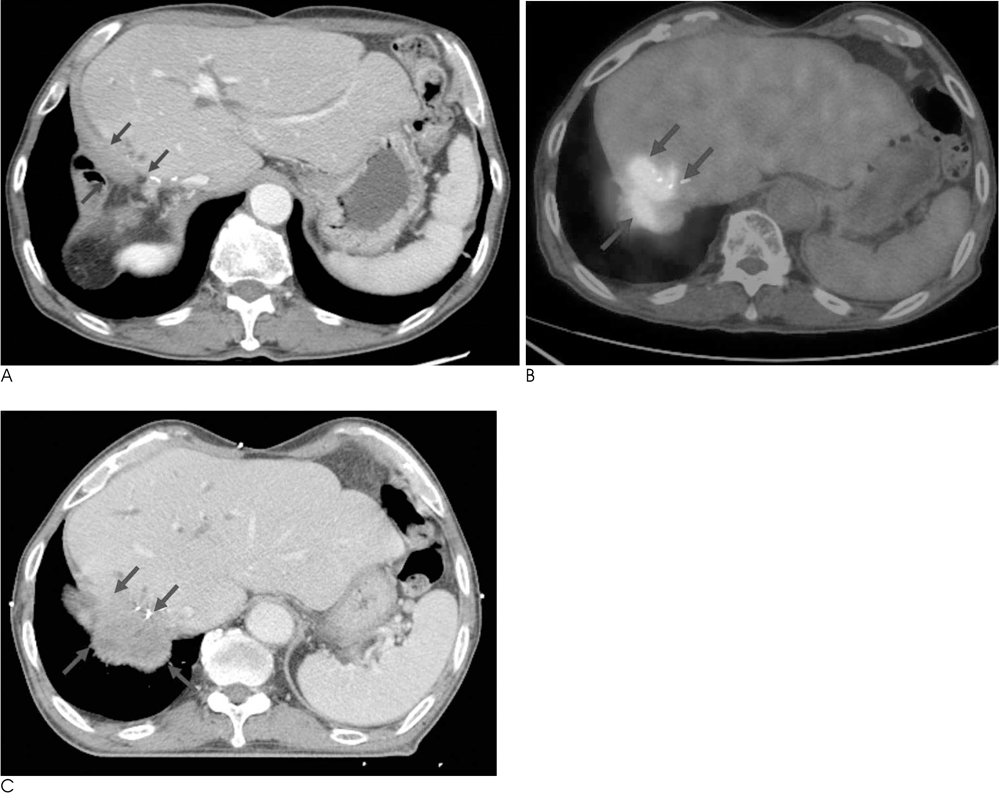
Fig. 2 Local recurrence in a 78-year-old man who had a history of right hepatectomy and Roux-en-Y hepaticojejunostomy for peripheral cholangiocarcinoma. A. Contrast-enhanced CT (CECT) shows no definite delineation of recurred mass at anastomotic site (arrows) in 1 years later after operation. B. Corresponding axial PET/CT demonstrate hypermetabolic lesion with SUV 9.1 (arrows), suggestive of recurred mass. C. Follow up CECT after 8 months, CECT shows irregular marginated heterogenously enhancing mass (arrows) at anastomotic site.

Fig. 3 Hepatic metastasis in a 71-year-old man who had a history of Whipple's operation for distal CBD cancer. A. Contrast-enhanced CT shows a about 3.5 cm heterogenous enhancing lesion (arrows) in hepatic dome. B. Corresponding axial PET/CT demonstrates focal hypermetabolic lesion (arrows) on hepatic dome.
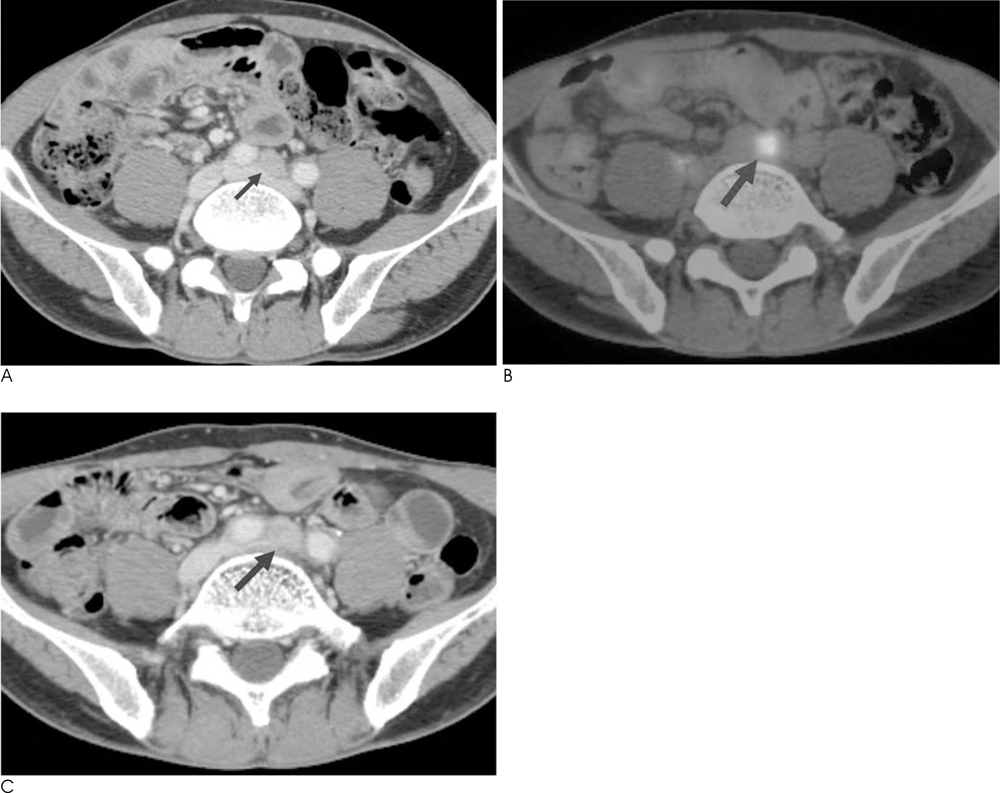
Fig. 4 Lymph node metastasis in a 53-year-old man who had a history of pylorus-preserving pancreatoduodenectomy (PPPD) for distal CBD cancer. A. Contrast-enhanced CT (CECT) shows a about 0.7 cm lymph node (arrow) around aortic bifurcation level, suggestive of benign lymph node. B. Corresponding axial PET/CT shows hypermetabolic metastatic lymph node (arrow) around aortic bifurcation level. C. Follow up CECT after 6 month reveals increased size of lymph node (arrow), suggestive of metastatic lymph node.
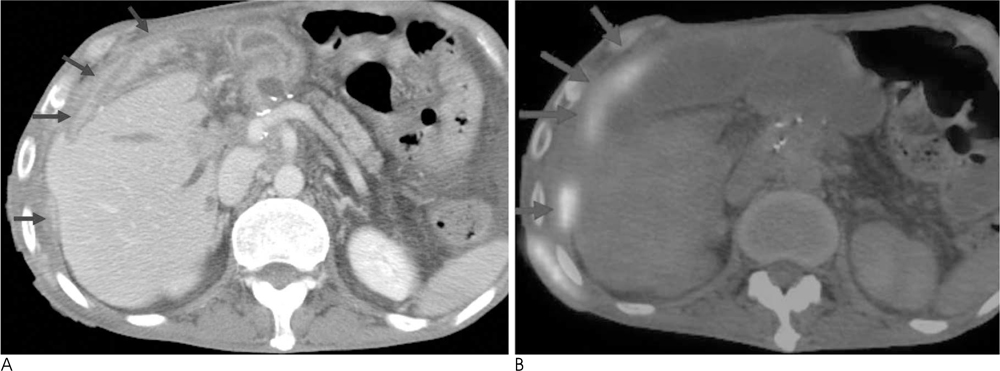
Fig. 5 Peritoneal seeding in a 54-year-old man who had a history of Whipple's operation for distal CBD cancer. A. Contrast-enhanced CT (CECT) shows irregular peritoneal thickening and scalloping of hepatic surface. B. Corresponding axial PET/CT shows hypermetabolic lesion in perihepatic space.
Reference
-
1. Nakajima T, Kondo Y, Miyazaki M, Okui K. A histopathologic study of 102 cases of intrahepatic cholangiocarcinoma: histologic classification and modes of spreading. Hum Pathol. 1988; 19:1228–1234.2. Lee DH, Kim DY, Lee SR. Radiological findings of bile duct carcinoma. J Korean Radiol Soc. 1982; 18:132–138.3. Klempnauer J, Ridder GJ, von Wasielewski R, Werner M, Weimann A, Pichlmayr R. Resectional surgery of hilar cholangiocarcinoma: a multivariate analysis of prognostic factors. J Clin Oncol. 1997; 15:947–954.4. Tsao JI, Nimura Y, Kamiya J, Hayakama N, Kondo S, Nagino M, et al. Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg. 2000; 232:166–174.5. Kostakoglu L, Agress H Jr, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer patients. Radiographics. 2003; 23:315–340.6. Rosenbaum SJ, Stergar H, Anotoch G, Bockisch A, Kuhl H. Staging and follow up of gastrointestinal tumors with PET-CT. Abdom Imaging. 2006; 31:25–35.7. Kostakoglu L, Hardoff R, Goldsmith SJ, Mirtcheva R. PET-CT fusion imaging in differentiating physiologic from pathologic FDG uptake. Radiographics. 2004; 24:1411–1431.8. Paudyal B, Oriuchi N, Paudyal P, Higuchi T, Nakajima T, Endo K. Expression of glucose transporters and hexokinase II in cholangiocellular carcinoma compared using [18F]-2-fluro-2-deoxy-D-glucose positron emission tomography. Cancer Sci. 2008; 99:260–266.9. Kim YJ, Yun M, Lee WJ, Kim KS, Lee JD. Usefulness of 18F-FDG PET in intrahepatic cholangiocarcinoma. EUR J Nucl Med Mol Imaging. 2003; 30:1467–1672.10. Tompkins RK, Thomas D, Wile A, Longmire WP Jr. Prognostic factors in bile duct carcinoma: analysis of 96 cases. Ann Surg. 1981; 194:447–457.11. Kosuge T, Yamamoto J, Shimada K, Yamasaki S, Makuuchi M. Improved surgical results for hilar cholangiocarcinoma with procedures including major hepatic resection. Ann Surg. 1999; 230:663–671.12. Kitagawa D, Taketoma A, Aishima S, Kuroda Y, Gion T, Shirabe K, et al. Recurrence of intrahepatic cholangiocarcinoma nine years after surgical resection. Hepatogastroenterology. 2008; 55:1085–1088.13. Jarnagin WR, Ruo L, Little SA, Klimstra D, D'Angelica M, Dematteo R, et al. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma: implications for adjuvant therapeutic strategies. Cancer. 2003; 98:1689–1700.14. Keogan MT, Seabourn JT, Paulson EK, Mcdermott VG, Delong DM, Nelson RC. Contrast-enhanced CT of intrahepatic and hilar cholangiocarcinoma: delay time for optimal imaging. AJR Am J Roentgenol. 1997; 169:1493–1499.15. Jadvar H, Henderson RW, Conti PS. [F-18]fluorodeoxyglucose positron emission tomography and positron emission tomography: computed tomography in recurrent and metastatic cholangiocarcinoma. J Comput Assist Tomogr. 2007; 31:223–228.16. Nakamoto Y, Sakamoto S, Okada T, Senda M, Higashi T, Saga T, et al. Clinical value of manual fusion of PET and CT images in patients with suspected recurrent colorectal cancer. AJR Am J Roentgenol. 2007; 188:257–267.17. Berger KL, Nicholson SA, Dehdashti F, Siegel BA. FDG PET evaluation of mucinous neoplasms: correlation of FDG uptake with histopathologic feature. AJR Am J Roentgenol. 2000; 174:1005–1008.18. Reinhardt MJ, Strunk H, Gerhardt T, Roedel R, Jaeger U, Bucerius J, et al. Detection of Klatskin's tumor in extrahepatic bile duct strictures using delayed 18F-FDG PET/CT: preliminary results for 22 patient studies. J Nucl Med. 2005; 46:1158–1163.19. Bipat S, van Leeuwen MS, Comans EF, Pijl ME, Bossuyt PM, Zwinderman AH, et al. Colorectal liver metastases: CT, MR imaging, and PET for diagnosis--meta-analysis. Radiology. 2005; 237:123–131.20. Einstein DM, Singer AA, Chilcote WA, Desai RK. Abdominal lymphadenopathy : spectrum of CT findings. Radiographics. 1991; 11:457–472.21. Chen LB, Tong JL, Song HZ, Zhu H, Wang YC. 18F-DG PET/CT in detection of recurrence and metastasis of colorectal cancer. World J Gastroenterol. 2007; 13:5025–5029.22. Park MJ, Lee WJ, Lim HK, Park KW, Choi JY, Kim BT. Detecting recurrence of gastric cancer: the value of FDG PET/CT. Abdom Imaging. 2008; Forthcoming.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
- Detecting the Recurrence of Gastric Cancer after Curative Resection: Comparison of FDG PET/CT and Contrast-Enhanced Abdominal CT
- The Role of 18F-FDG PET/CT in the Evaluation of Gastric Cancer Recurrence after Curative Gastrectomy
- Use of 18F-FDG PET/CT in Second Primary Cancer
