A Case of Adrenocortical Adenoma Causing Subclinical Cushing's Syndrome Mistaken for Liddle's Syndrome
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 2Department of Pathology, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2200664
- DOI: http://doi.org/10.3803/jkes.2006.21.1.58
Abstract
- Subclinical Cushing's syndrome is defined as an autonomous cortisol hyperproduction without specific clinical signs of cortisol excess, but detectable biochemically as derangements of the hypothalamic-pituitary-adrenal axis function. We report a case of a 33-year-old woman with subclinical Cushing's syndrome caused by left adrenocortical adenoma, mistaken for Liddle's syndrome. The patient complained of fatigue. Laboratory findings showed metabolic alkalosis, hypokalemia, high TTKG (transtubular K concentration gradient), low plasma renin activity, and low serum aldosterone level, that findings implied as Liddle's syndrome. So we performed further study. Hormonal and radiologic studies revealed subclinical Cushing's syndrome with a left adrenal mass. The adrenal mass was resected and pathologically diagnosed as adrenocortical adenoma. After the resection of the left adrenal mass, patient's hormonal levels showed normal range.
MeSH Terms
Figure
-
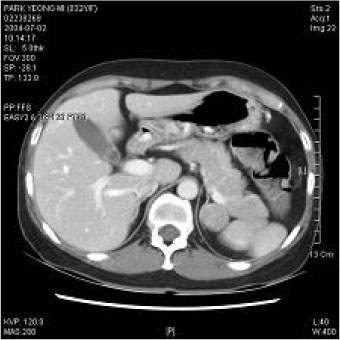
Fig. 1 Computed tomography of the abdomen showing 3 × 2 cm sized, oval shaped left adrenal mass.
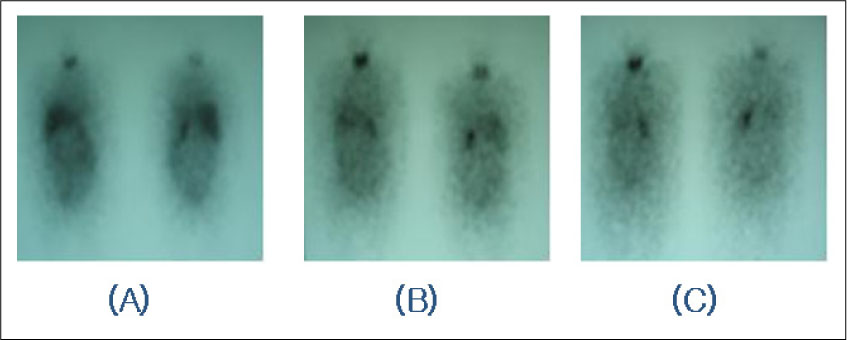
Fig. 2 Whole body scans were obtained 3 days (A), 5 days (B), 7 days (C) after injection of I-131 NP59 1 mCi. Adrenal scan [59-[131I]iodocholesterol scanning (NP59 scan)] showed nodular activity in the region of left adrenal gland.

Fig. 3 The tumor (3.2 × 3 × 2 cm sized) is well-circumscribed and bright yellow in color.

Fig.4 Microscopic finding of the tumor. (A) The tumor is well defined and composed of clear cells and eosinophilic cells (H & E stain, × 20). (B) The tumor cells have abundant clear cytoplasm and a small round nucleus (H & E stain, × 200).
Cited by 1 articles
-
Missed Ipsilateral Adrenal Adenoma With Recurrent Hypercortisolism After Prior Left Adrenalectomy
Jihoon Kim, Hae Kyung Kim, Choon Hee Chung
J Korean Med Sci. 2022;37(39):e278. doi: 10.3346/jkms.2022.37.e278.
Reference
-
1. Charbonnel B, Chatal JF, Ozanne P. Does the corticoadrenal adenoma with "pre-Cushing's" syndrome exist? J Nucl Med. 1981. 22:1059–1061.2. Reincke M. Subclinical Cushing's syndrome. Endocrinol Metab Clin North Am. 2000. 29:43–56.3. Ross NS. Epidemiology of Cushing's syndrome and subclinical disease. Endocrinol Metab Clin North Am. 1994. 23:539–546.4. Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev. 1995. 16:460–484.5. Gross MD, Shapiro B. Clinical reveiw 50: Clinically silent adrenal masses. J Clin Endocrinol Metab. 1993. 77:885–888.6. Glazer HS, Weyman PJ, Sagel SS. Nonfunctioning adrenal masses: incidental discovery on computed tomography. Am J Roentgenol. 1982. 139:81–85.7. Prinz RA, Brooks MH, Churchill R, Graner JL, Lawrence AM, Paloyan E, Sparagana M. Incidental asymptomatic adrenal masses detected by computed tomographic scanning. Is operation required? JAMA. 1982. 248:701–704.8. McLeod MK, Thompson NW, Gross MD, Bondeson AG, Bondeson L. Sub-clinical Cushing's syndrome in patients with adrenal incidentalomas. Pitfalls in diagnosis and management. Am Surg. 1990. 56:398–403.9. Reincke M, Nieke J, Krestin GP, Saeger W, Allolio B, Winkelman W. Preclinical Cushing's syndrome in adrenal "incidentalomas": comparison with adrenal Cushing's syndrome. J Clin Endocrinol Metab. 1992. 75:826–832.10. Caplan RH, Strutt PJ, Wickuss GG. Subclinical hormone secretion by incidentally discovered adrenal masses. Arch Surg. 1994. 129:291–296.11. Osella G, Terzolo M, Boretta G, Magro G, Ali A, Piovesan A, Paccotti P, Angeli A. Endocrine evaluation of incidentally discovered adrenal masses (Incidentalomas). J Clin Endocrinol Metab. 1994. 79:1532–1539.12. Russi S, Blumenthal HT, Gray SH. Small adenomas of the adrenal cortex in hypertension and diabetes. Arch Intern Med. 1945. 76:284–291.13. Leibowitz G, Tsur A, Chayen SD, Salameh M, Raz I, Cerasi E, Gross DJ. Pre-clinical Cushing's syndrome. An unexpected frequent cause of poor glycemic control in obese diabetic patients. Clin Endocrinol (Oxf). 1996. 44:717–722.14. Sartorio A, Conti A, Ferrero S, Giambona S, Re T, Passini E, Ambrosi B. Evaluation of markers of bone and collagen turnover in patients with active and preclinical Cushing's syndrome and in patients with adrenal incidentaloma. Eur J Endocrinol. 1998. 138:146–152.15. Barzon L, Scaroni C, Sonino N, Fallo F, Gregianin M, Macri C. Incidentally discovered adrenal tumors: Endocrine and scintigraphic correlates. J Clin Endocrinol Metab. 1998. 83:55–62.16. Terzolo M, Ali A, Osella G, Cesario F, Paccotti P, Angeli A. Subclinical Cushing's syndrome in adrenal incidentaloma. . Clin Endocrinol(Oxf). 1998. 48:89–97.17. Barson L, Scaroni C, Sonino N, Fallo F, Paoletta A, Boscaro M. Risk factors and long-term follow-up of adrenal incidentalomas. J Clin Endocrinol Metab. 1999. 84:520–526.18. Siren J, Tervahartiala P, Sivula P, Haapiainen R. Natural course of adrenal incidentalomas: seven-year follow-up study. World J Surg. 2000. 24:579–582.19. Barzon L, Fallo F, Sonino N, Boscaro M. Development of Cushing's syndrome in patients with adrenal incidentaloma. Eur J Endocrinol. 2002. 146:61–66.20. Morioka M, Fujii T, Matsuki T, Jo Y, Kobayashi T, Tanaka H, Ohashi T, Kondo K. Preclinical Cushing's syndrome: report of seven cases and a review of the literature. Int J Urol. 2000. 7:126–132.21. Emral R, Uysal AR, Asik M, Gullu S, Corapcioglu D, Tonyukuk V, Erdogan G. Prevalence of subclinical Cushing's syndrome in 70 patients with adrenal incidentaloma: clinical, biochemical and surgical outcomes. Endocr J. 2003. 50:399–408.22. Linos DA, Vassibpoulos PP, Papadimitriou J, Tountas K. The surgical management of adrenal cortical carcinoma. Int Surg. 1986. 71:104–106.23. Tsuboi Y, Ishikawa S, Fujisawa G, Okada K, Saito T. Possible pre-Cushing's syndrome due to an adrenal adenoma incidentally discovered. Endocr J. 1995. 42:509–516.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Cushing's Syndrome caused by Adrenocortical Carcinoma
- Two Cases of Functioning Adrenocortical Adenoma
- A case of adrenocortical adenoma with primary hyperaldosteronism and subclinical Cushing's syndrome
- A Case of Adrenal Cystic Pheochromocytoma with Contralateral Adrenocortical Adenoma Causing Subclinical Cushing's Syndrome
- A Case of Black Adrenocortical Adenoma Causing Cushing's Syndrome with Contralateral Nonfuncioning Adenoma
