J Korean Med Assoc.
2012 Oct;55(10):996-1002. 10.5124/jkma.2012.55.10.996.
Anesthetic management of the bariatric surgery
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, School of Medicine, Ewha Womans University, Seoul, Korea. leehee@ewha.ac.kr
- KMID: 2192820
- DOI: http://doi.org/10.5124/jkma.2012.55.10.996
Abstract
- Obesity, that is, having a body mass index (BMI) >30 kg/m2, has increased dramatically and became the most single most common preventable cause of death in South Korea. In the end, obesity results in metabolic syndrome, which includes abdominal obesity, increased triglycerides, decreased high-density lipoprotein, hypertension, and impaired glucose tolerance. Nonsurgical methods for obesity treatments include dietary therapy, exercise counseling, behavioral therapy, psychiatric therapy, and pharmacotherapy. Surgical methods for obesity treatments, laparoscopic gastric banding and Roux-en-Y gastric bypass, are commonly performed for obese patients, particularly those with a BMI of 40 kg/m2 or at BMI more than 30 kg/m2 with accompanying diseases related to metabolic syndrome such as hypertension, type 2 diabetes, hypercholesterolemia, asthma, angina, other cardiopulmonary diseases, infertility, polycystic ovary, urinary incontinence, severe arthritis, or Pickwickian syndrome. Preoperative evaluation for bariatric surgery should focus on airway management, sleep apnea history, use of a continuous positive airway pressure device, and comorbid systemic diseases. Special consideration and pharmacokinetic knowledge is needed for the choice and dose of the anesthetic agents as well as postoperative pain control, patient monitoring, fluid intake, and surgical complications. Obesity is a disease. Appropriate surgical intervention and peri-operative anesthetic care for bariatric surgery will increase the safety and satisfaction of obese patients and will finally provide a better quality of life for our society.
Keyword
MeSH Terms
-
Airway Management
Anesthesia
Anesthetics
Arthritis
Asthma
Bariatric Surgery
Body Mass Index
Cause of Death
Continuous Positive Airway Pressure
Counseling
Exercise Therapy
Female
Gastric Bypass
Glucose
Humans
Hypercholesterolemia
Hypertension
Infertility
Lipoproteins
Monitoring, Physiologic
Obesity
Obesity Hypoventilation Syndrome
Obesity, Abdominal
Ovary
Pain, Postoperative
Quality of Life
Republic of Korea
Sleep Apnea Syndromes
Triglycerides
Urinary Incontinence
Anesthetics
Glucose
Lipoproteins
Triglycerides
Figure
-
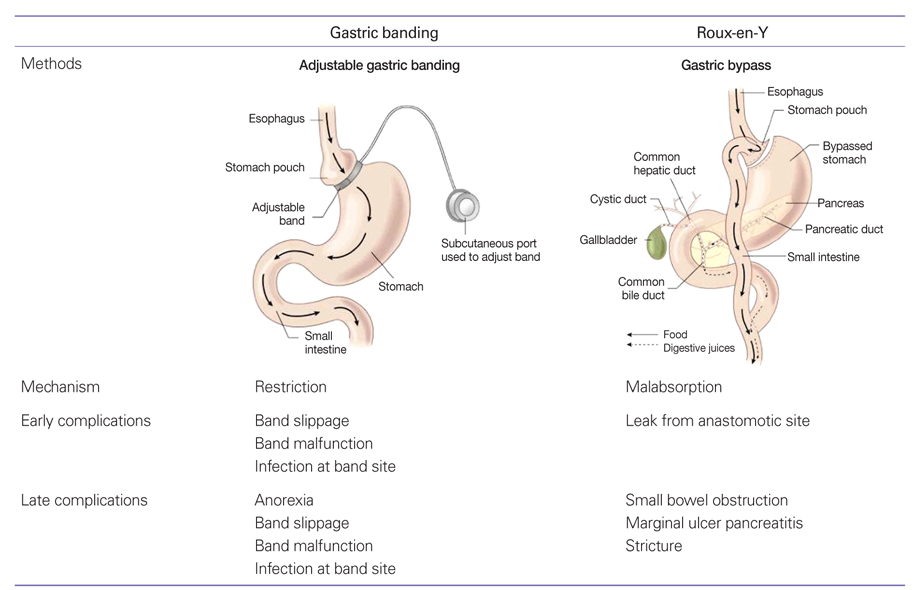
Figure 1 Complications after bariatric surgery.
Reference
-
1. Hubbard VS, Hall WH. Gastrointestinal surgery for severe obesity. Obes Surg. 1991. 1:257–265.2. Pories WJ, Dohm LG, Mansfield CJ. Beyond the BMI: the search for better guidelines for bariatric surgery. Obesity (Silver Spring). 2010. 18:865–871.
Article3. Hutter MM, Randall S, Khuri SF, Henderson WG, Abbott WM, Warshaw AL. Laparoscopic versus open gastric bypass for morbid obesity: a multicenter, prospective, risk-adjusted analysis from the National Surgical Quality Improvement Program. Ann Surg. 2006. 243:657–662.4. Gentileschi P, Kini S, Catarci M, Gagner M. Evidence-based medicine: open and laparoscopic bariatric surgery. Surg Endosc. 2002. 16:736–744.
Article5. Han SM, Kim WW. Early management of type 2 diabetes mellitus after sleeve gastrectomy in morbid obesity. J Korean Surg Soc. 2005. 69:304–309.6. Liberopoulos EN, Mikhailidis DP, Elisaf MS. Diagnosis and management of the metabolic syndrome in obesity. Obes Rev. 2005. 6:283–296.
Article7. Patil SP, Schneider H, Schwartz AR, Smith PL. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest. 2007. 132:325–337.8. Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg. 2008. 107:1543–1563.
Article9. Lopez-Jimenez F, Bhatia S, Collazo-Clavell ML, Sarr MG, Somers VK. Safety and efficacy of bariatric surgery in patients with coronary artery disease. Mayo Clin Proc. 2005. 80:1157–1162.
Article10. Collazo-Clavell ML, Clark MM, McAlpine DE, Jensen MD. Assessment and preparation of patients for bariatric surgery. Mayo Clin Proc. 2006. 81:10 Suppl. S11–S17.
Article11. Passannante AN, Rock P. Anesthetic management of patients with obesity and sleep apnea. Anesthesiol Clin North America. 2005. 23:479–491.
Article12. Bostanjian D, Anthone GJ, Hamoui N, Crookes PF. Rhabdomyolysis of gluteal muscles leading to renal failure: a potentially fatal complication of surgery in the morbidly obese. Obes Surg. 2003. 13:302–305.
Article13. Collier B, Goreja MA, Duke BE 3rd. Postoperative rhabdomyolysis with bariatric surgery. Obes Surg. 2003. 13:941–943.
Article14. Juvin P, Lavaut E, Dupont H, Lefevre P, Demetriou M, Dumoulin JL, Desmonts JM. Difficult tracheal intubation is more common in obese than in lean patients. Anesth Analg. 2003. 97:595–600.
Article15. Ezri T, Gewurtz G, Sessler DI, Medalion B, Szmuk P, Hagberg C, Susmallian S. Prediction of difficult laryngoscopy in obese patients by ultrasound quantification of anterior neck soft tissue. Anaesthesia. 2003. 58:1111–1114.
Article16. Jense HG, Dubin SA, Silverstein PI, O'Leary-Escolas U. Effect of obesity on safe duration of apnea in anesthetized humans. Anesth Analg. 1991. 72:89–93.
Article17. El-Dawlatly AA, Al-Dohayan A, Abdel-Meguid ME, El-Bakry A, Manaa EM. The effects of pneumoperitoneum on respiratory mechanics during general anesthesia for bariatric surgery. Obes Surg. 2004. 14:212–215.
Article18. Sprung J, Whalley DG, Falcone T, Wilks W, Navratil JE, Bourke DL. The effects of tidal volume and respiratory rate on oxygenation and respiratory mechanics during laparoscopy in morbidly obese patients. Anesth Analg. 2003. 97:268–274.
Article19. Egan TD, Huizinga B, Gupta SK, Jaarsma RL, Sperry RJ, Yee JB, Muir KT. Remifentanil pharmacokinetics in obese versus lean patients. Anesthesiology. 1998. 89:562–573.
Article20. Ogunnaike BO, Jones SB, Jones DB, Provost D, Whitten CW. Anesthetic considerations for bariatric surgery. Anesth Analg. 2002. 95:1793–1805.
Article21. De Baerdemaeker LE, Jacobs S, Den Blauwen NM, Pattyn P, Herregods LL, Mortier EP, Struys MM. Postoperative results after desflurane or sevoflurane combined with remifentanil in morbidly obese patients. Obes Surg. 2006. 16:728–733.
Article22. Illing L, Duncan PG, Yip R. Gastroesophageal reflux during anaesthesia. Can J Anaesth. 1992. 39(5 Pt 1):466–470.
Article23. Sharma SK, McCauley J, Cottam D, Mattar SG, Holover S, Dallal R, Lord J, Danner O, Ramanathan R, Eid G, Schauer P. Acute changes in renal function after laparoscopic gastric surgery for morbid obesity. Surg Obes Relat Dis. 2006. 2:389–392.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nutritional Management after Bariatric Surgery
- Dietary Management after Bariatric Surgery in Patients with Obesity and Diabetes
- 2018 Korean Society for Metabolic and Bariatric Surgery Guidelines
- Incidence and Management of Micronutrient Deficiencies in Post-bariatric Surgery Patients
- Enhanced Recovery after Surgery in Bariatric Surgery
