Natural Course of Initially Non-Operated Cases of Acute Subdural Hematoma : The Risk Factors of Hematoma Progression
- Affiliations
-
- 1Department of Neurosurgery, Gachon University, Gil Medical Center, Incheon, Korea. nschan@gilhospital.com
- KMID: 2190900
- DOI: http://doi.org/10.3340/jkns.2013.54.3.211
Abstract
OBJECTIVE
The objectives of the present study were to characterize the natural course of initially non-operated traumatic acute subdural hematoma (ASDH) and to identify the risk factors of hematoma progression.
METHODS
Retrospective analysis was performed using sequential computed tomography (CT) images maintained in a prospective observational database containing 177 ASDH cases treated from 2005 to 2011. Patients were allocated to four groups as followings; 136 (76.8%) patients to the spontaneous resolution group, 12 (6.8%) who underwent operation between 4 hours and 7 days to the rapid worsening group (RWG), 24 (13.6%) who experienced an increase of hematoma and that underwent operation between 7 and 28 days to the subacute worsening group (SWG), and 5 (2.8%) who developed delayed aggravation requiring surgery from one month after onset to the delayed worsening group (DWG). Groups were compared with respect to various factors.
RESULTS
No significant intergroup difference was found with respect to age, mechanism of injury, or initial Glasgow Coma Scale. The presence of combined cerebral contusion or subarachnoid hemorrhage was found to be a significant prognostic factor. Regarding CT findings, mixed density was common in the RWG and the SWG. Midline shifting, hematoma thickness, and numbers of CT slices containing hematoma were significant prognostic factors of the RWG and the SWG. Brain atrophy was more severe in the SWG and the DWG.
CONCLUSION
A large proportion of initially non-operated ASDHs worsen in the acute or subacute phase. Patients with risk factors should be monitored carefully for progression by repeat CT imaging.
MeSH Terms
Figure
-

Fig. 1 Longitudinal proportion of the largest hematoma was defined as the ratio of hematoma convexity to cerebral hemisphere convexity (A/B).
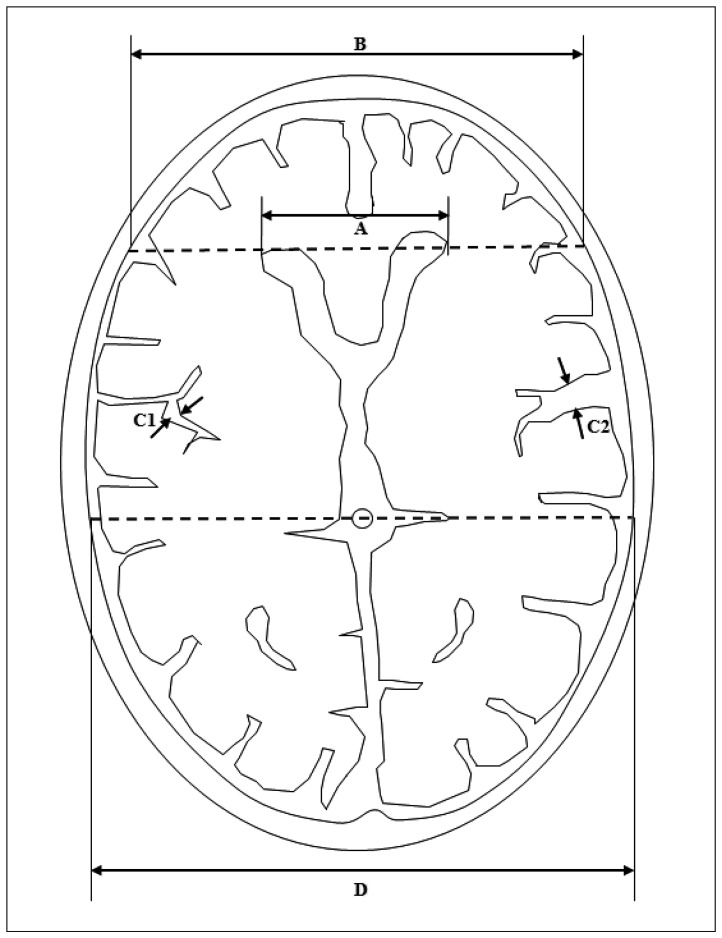
Fig. 2 Measurement of frontal horn index (FHI), and sylvian fissure ratio (SFR). A : Frontal horn diameter (FHD), the distance between the tips of the frontal horns measured on the CT section depicting them best. B : Innner table diameter (ITD), the distance between the inner tables of the skull measured on the same section, and along the same line used to measure FHD. C1 and C2 : Maximum widths of the two sylvian fissures. D : Transpineal coronal inner table diameter. FHI was defined as the ratio of FHD to ITD (A/B). SFR was defined as the average of the maximum width of the two sylvian fissures on the section showing them at their widest, divided by the transpineal coronal inner table diameter [(C1+C2)/2D]. If the sylvian fissure was not visible in the hematoma side, the contralateral side×2 was used.
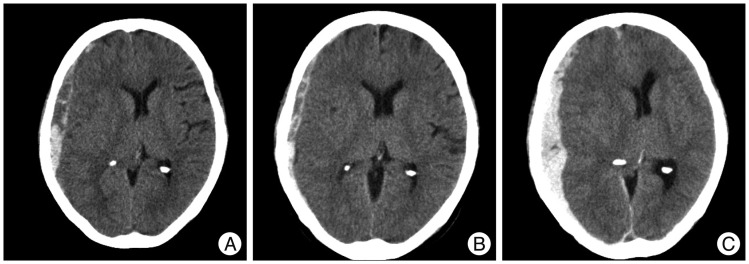
Fig. 3 Computed tomography (CT) scans showing an example of rapid worsening. A : Initial head CT reveals a mixed density, thick ASDH with cerebral contusion, traumatic SAH, and moderate midline shifting. B : Three hours later, head CT shows slight hematoma thinning and a midline shifting improvement. C : However, 3 days later, the patient showed a sudden neurologic deterioration (GCS score 8), and follow-up head CT reveals aggravated hematoma and midline shifting. Craniectomy was performed immediately. Her final GCS score was 10. ASDH : acute subdural hematoma, SAH : subarachnoid hemorrhage, GCS : Glasgow Coma Scale.
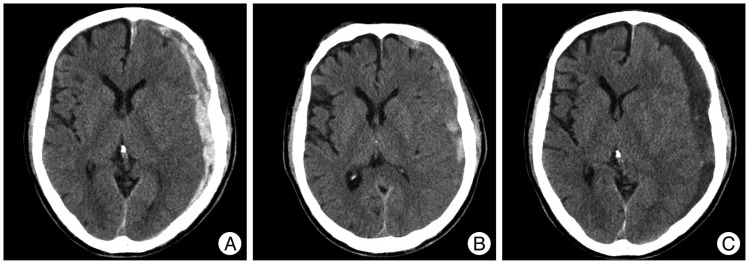
Fig. 4 Computed tomography (CT) scans showing an example of subacute worsening. A : Initial head CT reveals a mixed density, thick ASDH with mild midline shifting with moderate brain atrophy. B : One week later, head CT shows hematoma resolution transiently. C : However, at 2 weeks after admission, his symptoms worsened gradually to GCS score 10. Follow-up head CT reveals low-density subdural fluid collection with severe midline shifting. Trephination surgery was performed, and fortunately, his final GCS score recovered to 14. ASDH : acute subdural hematoma, GCS : Glasgow Coma Scale.

Fig. 5 Computed tomography (CT) scans showing an example of delayed worsening. A : Initial head CT reveals a homogeneous density ASDH in the right frontal and interhemispheric fissure. B : Two weeks later, head CT shows hematoma resolution but progression of bilateral subdural hygroma. C : Three months later, follow-up head CT reveals hydrocephalus and a ventriculo-peritoneal shunt procedure was performed. ASDH : acute subdural hematoma.
Cited by 1 articles
-
Impact of Time Interval between Trauma Onset and Burr Hole Surgery on Recurrence of Late Subacute or Chronic Subdural Hematoma
Dae-in Kim, Jae-hoon Kim, Hee-in Kang, Byung-gwan Moon, Joo-seung Kim, Deok-ryeong Kim
J Korean Neurosurg Soc. 2016;59(5):498-504. doi: 10.3340/jkns.2016.59.5.498.
Reference
-
1. Aoki N. Acute subdural haematoma with rapid resolution. Acta Neurochir (Wien). 1990; 103:76–78. PMID: 2360472.
Article2. Barkley JM, Morales D, Hayman LA, Diaz-Marchan PJ. Static neuroimaging in the evaluation of TBI. In : Zasler ND, Katz DI, Zafonte RD, editors. Brain Injury Medicine : Principles and Practice. New York: Demos;2007. p. 129–148.3. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, et al. Surgical management of acute subdural hematomas. Neurosurgery. 2006; 58(3 Suppl):S16–S24. discussion Si-Siv. PMID: 16710968.
Article4. Cardoso ER, Schubert R. External hydrocephalus in adults. Report of three cases. J Neurosurg. 1996; 85:1143–1147. PMID: 8929508.5. Chang EF, Meeker M, Holland MC. Acute traumatic intraparenchymal hemorrhage : risk factors for progression in the early post-injury period. Neurosurgery. 2007; 61(1 Suppl):222–230. discussion 230-231. PMID: 18813167.6. Chieregato A, Fainardi E, Morselli-Labate AM, Antonelli V, Compagnone C, Targa L, et al. Factors associated with neurological outcome and lesion progression in traumatic subarachnoid hemorrhage patients. Neurosurgery. 2005; 56:671–680. discussion 671-680. PMID: 15792505.
Article7. Dent DL, Croce MA, Menke PG, Young BH, Hinson MS, Kudsk KA, et al. Prognostic factors after acute subdural hematoma. J Trauma. 1995; 39:36–42. discussion 42-43. PMID: 7636908.
Article8. Feliciano CE, De Jesús O. Conservative management outcomes of traumatic acute subdural hematomas. P R Health Sci J. 2008; 27:220–223. PMID: 18782966.9. Gean AD. Imaging of head Trauma. Philadelphia: Lippincott Williams & Wilkins;1994.10. Greenberg J, Cohen WA, Cooper PR. The "hyperacute" extraaxial intracranial hematoma : computed tomographic findings and clinical significance. Neurosurgery. 1985; 17:48–56. PMID: 4022287.
Article11. Huh PW, Yoo DS, Cho KS, Park CK, Kang SG, Park YS, et al. Diagnostic method for differentiating external hydrocephalus from simple subdural hygroma. J Neurosurg. 2006; 105:65–70. PMID: 16874890.
Article12. Izumihara A, Orita T, Tsurutani T, Kajiwara K. [Natural course of non-operative cases of acute subdural hematoma : sequential computed tomographic study in the acute and subacute stages]. No Shinkei Geka. 1997; 25:307–314. PMID: 9125713.13. Kawamata T, Takeshita M, Kubo O, Izawa M, Kagawa M, Takakura K. Management of intracranial hemorrhage associated with anticoagulant therapy. Surg Neurol. 1995; 44:438–442. discussion 443. PMID: 8629228.
Article14. Kim H, Shim YB, Chung DJ, Kim SM, Park YK, Choi SK. Rapid spontaneous resolution of acute subdural hematoma. J Korean Neurosurg Soc. 1999; 28:1636–1638.15. Lee CH, Kang DH, Hwang SH, Park IS, Jung JM, Han JW. Spontaneous rapid reduction of a large acute subdural hematoma. J Korean Med Sci. 2009; 24:1224–1226. PMID: 19949689.
Article16. Lee KS, Bae WK, Bae HG, Yun IG. The fate of traumatic subdural hygroma in serial computed tomographic scans. J Korean Med Sci. 2000; 15:560–568. PMID: 11068995.
Article17. Lee KS, Bae WK, Park YT, Yun IG. The pathogenesis and fate of traumatic subdural hygroma. Br J Neurosurg. 1994; 8:551–558. PMID: 7857535.
Article18. Lee KS, Shim JJ, Yoon SM, Doh JW, Yun IG, Bae HG. Acute-on-chronic subdural hematoma : not uncommon events. J Korean Neurosurg Soc. 2011; 50:512–516. PMID: 22323938.
Article19. Mathew P, Oluoch-Olunya DL, Condon BR, Bullock R. Acute subdural haematoma in the conscious patient : outcome with initial non-operative management. Acta Neurochir (Wien). 1993; 121:100–108. PMID: 8512003.
Article20. Matsuyama T, Shimomura T, Okumura Y, Sakaki T. Acute subdural hematomas due to rupture of cortical arteries : a study of the points of rupture in 19 cases. Surg Neurol. 1997; 47:423–427. PMID: 9131022.
Article21. Matsuyama T, Shimomura T, Okumura Y, Sakaki T. Rapid resolution of symptomatic acute subdural hematoma : case report. Surg Neurol. 1997; 48:193–196. PMID: 9242248.22. Oertel M, Kelly DF, McArthur D, Boscardin WJ, Glenn TC, Lee JH, et al. Progressive hemorrhage after head trauma : predictors and consequences of the evolving injury. J Neurosurg. 2002; 96:109–116. PMID: 11794591.
Article23. Okumura Y, Shimomura T, Park YS. [A study of acute subdural hematoma developing into hematoma with capsule formation]. No Shinkei Geka. 1998; 26:691–698. PMID: 9743998.24. Park SH, Kang DH, Park J, Hwang JH, Hwang SK, Sung JK, et al. Fibrinogen and D-dimer analysis of chronic subdural hematomas and computed tomography findings : a prospective study. Clin Neurol Neurosurg. 2011; 113:272–276. PMID: 21156338.
Article25. Patel NY, Hoyt DB, Nakaji P, Marshall L, Holbrook T, Coimbra R, et al. Traumatic brain injury : patterns of failure of nonoperative management. J Trauma. 2000; 48:367–374. discussion 374-375. PMID: 10744271.26. Servadei F, Antonelli V, Giuliani G, Fainardi E, Chieregato A, Targa L. Evolving lesions in traumatic subarachnoid hemorrhage : prospective study of 110 patients with emphasis on the role of ICP monitoring. Acta Neurochir Suppl. 2002; 81:81–82. PMID: 12168364.27. St John JN, Dila C. Traumatic subdural hygroma in adults. Neurosurgery. 1981; 9:621–626. PMID: 7322326.
Article28. Stein SC, Young GS, Talucci RC, Greenbaum BH, Ross SE. Delayed brain injury after head trauma : significance of coagulopathy. Neurosurgery. 1992; 30:160–165. PMID: 1545882.29. Wu MC, Liu JX, Luo GC, Zhang ZW, Min J, Yu H, et al. Rapid natural resolution of intracranial hematoma. Chin J Traumatol. 2004; 7:96–100. PMID: 15294128.30. Yang AI, Balser DS, Mikheev A, Offen S, Huang JH, Babb J, et al. Cerebral atrophy is associated with development of chronic subdural haematoma. Brain Inj. 2012; 26:1731–1736. PMID: 22759238.
Article31. Zanini MA, de Lima Resende LA, de Souza Faleiros AT, Gabarra RC. Traumatic subdural hygromas : proposed pathogenesis based classification. J Trauma. 2008; 64:705–713. PMID: 18332811.32. Zwienenberg-Lee M, Muizelaar JP. Clinical pathophysiology of traumatic brain injury. In : Winn HR, Youmans JR, editors. Youmans Neurological Surgery. Philadelphia, PA: WB Saunders;2011. p. 3335–3370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
- Risk Factors of Chronic Subdural Hematoma Progression after Conservative Management of Cases with Initially Acute Subdural Hematoma
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Spontaneously Rapid Resolution of Acute Subdural Hemorrhage with Severe Midline Shift
