Risk Factors of Chronic Subdural Hematoma Progression after Conservative Management of Cases with Initially Acute Subdural Hematoma
- Affiliations
-
- 1Department of Neurosurgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. cs8.choi@samsung.com
- KMID: 2378258
- DOI: http://doi.org/10.13004/kjnt.2015.11.2.52
Abstract
OBJECTIVE
Acute subdural hematoma (ASDH) patients are treated conservatively or surgically according to the guidelines for surgical treatment. Many patients with thin ASDH and mild neurologic deficit are managed conservatively, but sometimes aggravation of thin ASDH to chronic subdural hematoma (CSDH) results in exacerbated clinical symtoms and consequently requires surgery. The aim of this study is to evaluate risk factors that indicate progression of initially non-operated ASDH to CSDH.
METHODS
We divided 177 patients, presenting with ASDH (managed conservatively initially) between January 2008 to December 2013, into two groups; 'CSDH progression group' (n=16) and 'non-CSDH progression group' (n=161). Patient's data including age, sex, past medical history, medication were collected and brain computed tomography was used for radiologic analysis.
RESULTS
Our data demonstrated that no significant intergroup difference with respect to age, sex ratio, co-morbid conditions, medication history, ischemic heart disease, liver disease and end-stage renal disease was found. However, Hounsfield unit (hematoma density) and mixed density was higher in the 'ASDH progression group' (67.50+/-7.63) than in the 'non-CSDH progression group' (61.53+/-10.69) (p=0.031). Midline shifting and hematoma depth in the 'CSDH progression group' were significantly greater than the 'non-CSDH progression group' (p=0.067, p=0.005).
CONCLUSION
Based on the results of this study, the risk factors that are related to progression of initially non-operated ASDH to CSDH are higher Hounsfield unit and hematoma depth. Therefore, we suggest that ASDH patients, who have bigger hematoma depth and higher Hounsfield unit, should be monitored and managed carefully during the follow-up period.
MeSH Terms
Figure
-
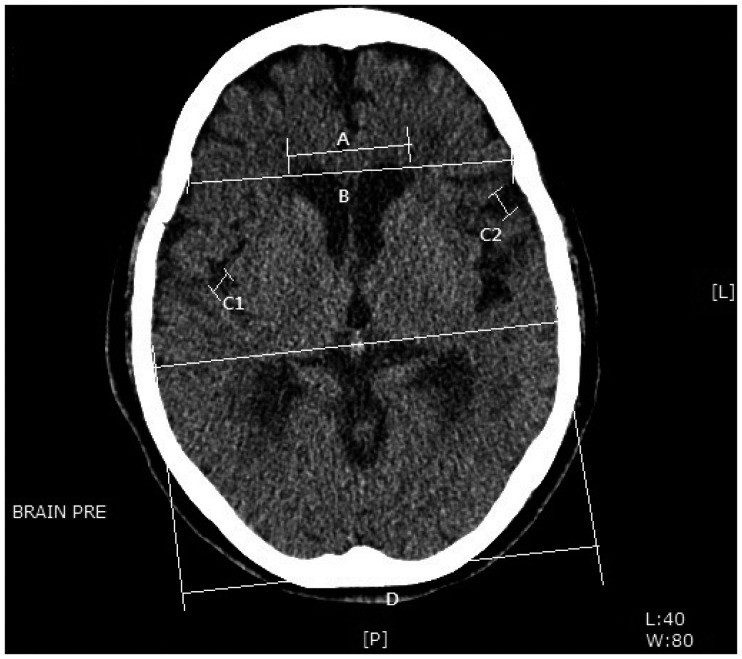
FIGURE 1 Measurement of brain atrophy using 'frontal horn index (FHI)' and 'sylvian fissure ratio (SFR)'. First, FHI is the ratio of 'A' (distance between two frontal horns) and 'B' (distance of inner table). Second, SFR is calculated with the equation of '(C1+C2)/D'.
Cited by 3 articles
-
Correlation between Head Trauma and Outcome of Chronic Subdural Hematoma
Dong Han Kim, Eun Suk Park, Min Soo Kim, Sung Ho Park, Jun Bum Park, Soon Chan Kwon, In Uk Lyo, Hong Bo Sim
Korean J Neurotrauma. 2016;12(2):94-100. doi: 10.13004/kjnt.2016.12.2.94.Delayed Burr Hole Surgery in Patients with Acute Subdural Hematoma: Clinical Analysis
Yoon Heuck Choi, Seong Rok Han, Chang Hyun Lee, Chan Young Choi, Moon Jun Sohn, Chae Heuck Lee
J Korean Neurosurg Soc. 2017;60(6):717-722. doi: 10.3340/jkns.2017.0404.010.Risk Factors of Delayed Surgical Intervention after Conservatively Treated Acute Traumatic Subdural Hematoma
Hyungjoo Kwon, Kyu-Sun Choi, Hyeong-Joong Yi, Hyoung-Joon Chun, Young-Jun Lee, Dong-won Kim
J Korean Neurosurg Soc. 2017;60(6):723-729. doi: 10.3340/jkns.2017.0506.011.
Reference
-
1. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, et al. Surgical management of acute subdural hematomas. Neurosurgery. 2006; 58(3 Suppl):S16–S24. discussion Si-SivPMID: 16710968.
Article2. Drapkin AJ. Chronic subdural hematoma: pathophysiological basis for treatment. Br J Neurosurg. 1991; 5:467–473. PMID: 1764228.
Article3. Feliciano CE, De Jesús O. Conservative management outcomes of traumatic acute subdural hematomas. P R Health Sci J. 2008; 27:220–223. PMID: 18782966.4. Kalanithi P, Schubert RD, Lad SP, Harris OA, Boakye M. Hospital costs, incidence, and inhospital mortality rates of traumatic subdural hematoma in the United States. J Neurosurg. 2011; 115:1013–1018. PMID: 21819196.
Article5. Karibe H, Hayashi T, Hirano T, Kameyama M, Nakagawa A, Tominaga T. Surgical management of traumatic acute subdural hematoma in adults: a review. Neurol Med Chir (Tokyo). 2014; 54:887–894. PMID: 25367584.
Article6. Ko BS, Lee JK, Seo BR, Moon SJ, Kim JH, Kim SH. Clinical analysis of risk factors related to recurrent chronic subdural hematoma. J Korean Neurosurg Soc. 2008; 43:11–15. PMID: 19096538.
Article7. Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006; 21:375–378. PMID: 16983222.8. Laviv Y, Rappaport ZH. Risk factors for development of significant chronic subdural hematoma following conservative treatment of acute subdural hemorrhage. Br J Neurosurg. 2014; 28:733–738. PMID: 24836959.
Article9. Lindvall P, Koskinen LO. Anticoagulants and antiplatelet agents and the risk of development and recurrence of chronic subdural haematomas. J Clin Neurosci. 2009; 16:1287–1290. PMID: 19564115.
Article10. Mathew P, Oluoch-Olunya DL, Condon BR, Bullock R. Acute subdural haematoma in the conscious patient: outcome with initial non-operative management. Acta Neurochir(Wien). 1993; 121:100–108. PMID: 8512003.
Article11. Rust T, Kiemer N, Erasmus A. Chronic subdural haematomas and anticoagulation or anti-thrombotic therapy. J Clin Neurosci. 2006; 13:823–827. PMID: 16997707.
Article12. Servadei F, Nasi MT, Cremonini AM, Giuliani G, Cenni P, Nanni A. Importance of a reliable admission Glasgow Coma Scale score for determining the need for evacuation of posttraumatic subdural hematomas: a prospective study of 65 patients. J Trauma. 1998; 44:868–873. PMID: 9603091.13. Shima K, Aruga T, Onuma T, Shigemori M. members of the Japanese Guidelines Committee on the Management of Severe Head Injury (2nd Edition), and the Japan Society of Neurotraumatology. JSNT-Guidelines for the Management of Severe Head Injury (Abridged edition). Asian J Neurosu. 2010; 5:15–23.14. Son S, Yoo CJ, Lee SG, Kim EY, Park CW, Kim WK. Natural course of initially non-operated cases of acute subdural hematoma: the risk factors of hematoma progression. J Korean Neurosurg Soc. 2013; 54:211–219. PMID: 24278650.15. Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S. Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery. 2008; 63:1125–1129. discussion 1129PMID: 19008766.16. Yamashima T, Yamamoto S. Clinicopathological study of acute subdural haematoma in the chronic healing stage. Clinical, histological and ultrastructural comparisons with chronic subdural haematoma. Neurochirurgia (Stuttg). 1984; 27:98–105. PMID: 6483072.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
- Spontaneously Rapid Resolution of Acute Subdural Hemorrhage with Severe Midline Shift
- Treatment of Chronic Subdural Hematoma with Arachnoid Cyst
