Comparison between Lateral Supraorbital Approach and Pterional Approach in the Surgical Treatment of Unruptured Intracranial Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. nsdrckc@naver.com
- KMID: 2190486
- DOI: http://doi.org/10.3340/jkns.2012.51.6.334
Abstract
OBJECTIVE
The lateral supraorbital (LSO) approach is a modified method of the classic pterional approach and it has advantages of short skin incision and small craniotomy compared with the pterional approach. This study was designed to compare the two approaches in the surgical treatment of unruptured intracranial aneurysms.
METHODS
We retrospectively reviewed 122 patients with 137 unruptured intracranial aneurysms treated by clipping, from July 2009 to April 2011. Between August 2010 and April 2011, 61 patients were treated by clipping via the lateral supraorbital approach and the same number of patients treated by clipping via the pterional approach were retrospectively enrolled. We analyzed the two groups and compared demographic, radiologic and clinical variables.
RESULTS
The mean age of patients in the two groups was 54.6 years (LSO group) and 55.7 years (Pterion group). The mean duration of hospitalization was shorter in the LSO group than in the Pterion group (7.9 days vs. 9.0 days, p=0.125) and the mean operation time was also significantly shorter in the LSO group (117.1 minutes vs. 164.3 minutes, p<0.001). Furthermore, the mean craniotomy area was much smaller in the LSO group (1275.4 mm2 vs. 2858.9 mm2, p<0.001). The two groups showed similar distributions of aneurysm location and postoperative complications.
CONCLUSION
The lateral supraorbital approach for the clipping of unruptured intracranial aneurysm could be a good alternative to the classic pterional approach.
Keyword
Figure
-
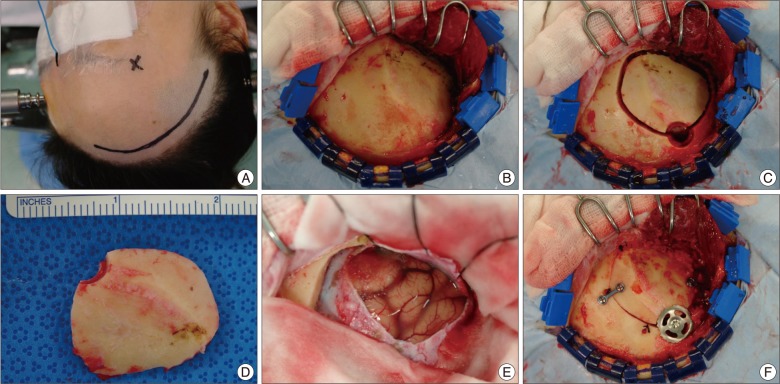
Fig. 1 The skin incision is usually behind the hair line and did not even go down in front of the ear to the level of zygomatic arch (A). The one layer skin-galea-muscle flap is dislocated after detachment from the bone by periosteal elevator and diathermy, and the flap is retracted anteriorly with spring hooks (B). Only one burr hole is made posteriorly and the bone flap is detached mainly by side-cutting craniotome with the basal part drilled off before lifting the flap (C). The bone flap size is about 3×4 cm (D). The dura mater is opened in a curvilinear incision pointing anterolaterally and elevated with stitches (E). After aneurysm clipping, the bone flap is secured using one skull fixator and two plate and screw systems (F).
Cited by 8 articles
-
The Usefulness of the Frontolateral Approach as a Minimally Invasive Corridor for Clipping of Anterior Circulation Aneurysm
Jeyul Yang, Chang Wan Oh, O-Ki Kwon, Gyojun Hwang, Tackeun Kim, Jong Un Moon, Seong Yeol Ahn, Jun Hak Kim, Jinseong Kim, Jae Seung Bang
J Cerebrovasc Endovasc Neurosurg. 2014;16(3):235-240. doi: 10.7461/jcen.2014.16.3.235.Clipping of Incidental Aneurysm of Middle Cerebral Artery Through Small Temporal Craniotomy and Linear Skin Incision
Jong Hyun Mun, Kyu Yong Cho, Rae Seop Lee, Byung Chan Lim, Tai Min Choi, Jun Seob Lim
J Cerebrovasc Endovasc Neurosurg. 2014;16(1):32-38. doi: 10.7461/jcen.2014.16.1.32.Modified Arachnoid Plasty Reduces Chronic Subdural Hematoma after Unruptured Aneurysm Clipping : Technical Note
Won Jae Lee, Taek Min Nam, Kyung-Il Jo, Je Young Yeon, Seung-Chyul Hong, Jong-Soo Kim
J Korean Neurosurg Soc. 2018;61(6):761-766. doi: 10.3340/jkns.2017.0242.Incidence and Risk Factors of Chronic Subdural Hematoma after Surgical Clipping for Unruptured Anterior Circulation Aneurysms
Won Jae Lee, Kyung-Il Jo, Je Young Yeon, Seung-Chyul Hong, Jong-Soo Kim
J Korean Neurosurg Soc. 2015;57(4):271-275. doi: 10.3340/jkns.2015.57.4.271.Feasibility and Efficacy of Olfactory Protection Using Gelfoam and Fibrin Glue during Anterior Communicating Artery Aneurysm Surgery
Hoyeon Cho, Kyung-Il Jo, Je Young Yeon, Seung-Chyul Hong, Jong-Soo Kim
J Korean Neurosurg Soc. 2015;58(2):107-111. doi: 10.3340/jkns.2015.58.2.107.Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
Won-Sang Cho, Jeong Eun Kim, Hyun-Seung Kang, Young-Je Son, Jae Seung Bang, Chang Wan Oh
J Korean Neurosurg Soc. 2017;60(3):275-281. doi: 10.3340/jkns.2017.0101.002.Keyhole approach in anterior circulation aneurysm: Current indication, advantages, technical limitations, complications and their avoidance
Hanuman Prajapati, Ahmad Ansari, Manish Jaiswal
J Cerebrovasc Endovasc Neurosurg. 2022;24(2):101-112. doi: 10.7461/jcen.2022.E2021.07.008.“Island Hole” Dural Tenting Suture on the Temporal Craniotomy for the Prevention of Epidural Hemorrhage in the Surgical Treatment of Unruptured Intracranial Aneurysms
Minchang Kim, In-Chul Yang, Bum-Tae Kim
J Korean Neurosurg Soc. 2024;67(1):130-132. doi: 10.3340/jkns.2023.0132.
Reference
-
1. Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, et al. The minipterional craniotomy : technical description and anatomic assessment. Neurosurgery. 2007; 61:256–264. discussion 264-265. PMID: 18091240.2. Figueiredo EG, Deshmukh V, Nakaji P, Deshmukh P, Crusius MU, Crawford N, et al. An anatomical evaluation of the mini-supraorbital approach and comparison with standard craniotomies. Neurosurgery. 2006; 59:ONS212–ONS220. discussion ONS220. PMID: 17041490.
Article3. Hernesniemi J, Ishii K, Niemelä M, Smrcka M, Kivipelto L, Fujiki M, et al. Lateral supraorbital approach as an alternative to the classical pterional approach. Acta Neurochir Suppl. 2005; 94:17–21. PMID: 16060236.
Article4. Mori K, Yamamoto T, Nakao Y, Oyama K, Esaki T, Watanabe M, et al. Lateral supraorbital keyhole approach to clip unruptured anterior communicating artery aneurysms. Minim Invasive Neurosurg. 2008; 51:292–297. PMID: 18855295.
Article5. Oikawa S, Mizuno M, Muraoka S, Kobayashi S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy. Technical note. J Neurosurg. 1996; 84:297–299. PMID: 8592239.
Article6. Park JC, Hamm IS. Cortical osteotomy technique for mobilizing the temporal muscle in pterional craniotomies. Technical note. J Neurosurg. 2005; 102:174–178. PMID: 15658112.
Article7. Salma A, Alkandari A, Sammet S, Ammirati M. Lateral supraorbital approach versus pterional approach : an anatomical qualitative and quantitative evaluation. Neurosurgery. 2011; 68:364–372. PMID: 21336206.8. Steiger HJ, Schmid-Elsaesser R, Stummer W, Uhl E. Transorbital keyhole approach to anterior communicating artery aneurysms. Neurosurgery. 2001; 48:347–351. discussion 351-352. PMID: 11220378.
Article9. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms : concept and technique. Surg Neurol. 1998; 49:481–489. discussion 489-490. PMID: 9586924.10. Wen HT, de Oliveira E, Tedeschi H, Andrade FC, Rhoton AL. The pterional approach : surgical anatomy, operative technique, and rationale. Oper Tech Neurosurg. 2001; 4:60–72.
Article11. Yasargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol. 1975; 3:7–14. PMID: 1111150.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microsurgical Experience with Supraorbital Keyhole Operations on Anterior Circulation Aneurysms
- Unruptured Supraclinoid Internal Carotid Artery Aneurysm Surgery : Superciliary Keyhole Approach versus Pterional Approach
- Supraorbital Keyhole Approach for Intracranial Aneurysms : Transitioning from Concerns to Confidence
- Pterional-subolfactory Approach for Treatment of High Positioned Anterior Communicating Artery Aneurysms
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
