Supraorbital Keyhole Approach for Intracranial Aneurysms : Transitioning from Concerns to Confidence
- Affiliations
-
- 1Department of Neurosurgery and Biomedical Research Institute, School of Medicine, Kyungpook National University, Daegu, Korea
- KMID: 2501688
- DOI: http://doi.org/10.3340/jkns.2019.0042
Abstract
- For surgical minimalism to reduce iatrogenic traumatization, a supraorbital keyhole approach has already been successfully applied to treat many unruptured anterior circulation aneurysms. However, using this minimal approach also raises several technical concerns due to the small cranial opening and cosmetic impact of a facial incision. Yet, such technical limitations can be overcome by using favorable surgical indications, slender surgical instruments, and optimized surgical techniques, while excellent cosmetic outcomes can be achieved using a short skin incision located <1 cm from the supraorbital margin, reconstruction of any bone defects around the bone flap, and meticulous wound closure. Thus, given such reassuring surgical results, in terms of the clipping status, neurological effects, and cosmetic outcomes, any concerns can be transitioned into confidence.
Figure
-
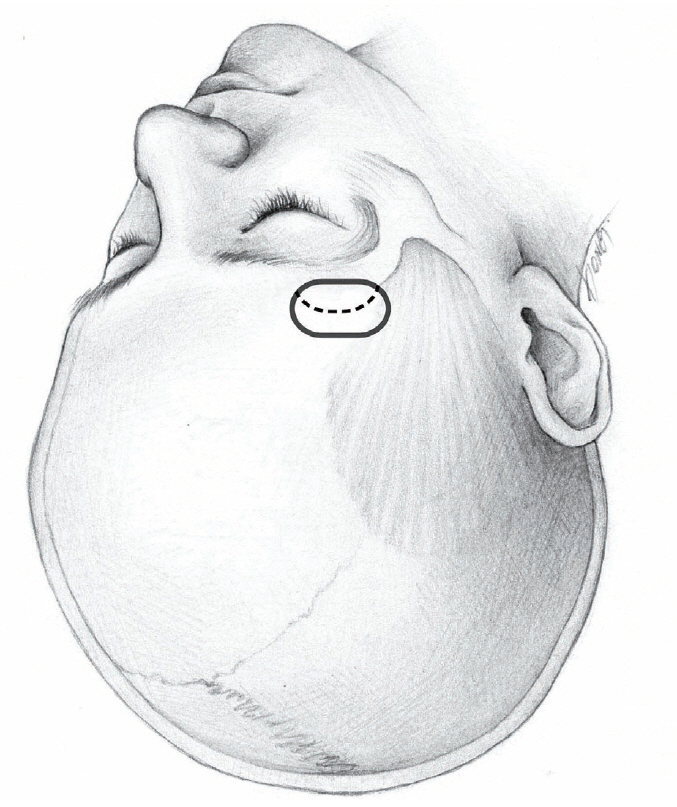
Fig. 1. Cranial opening for ICA and ACoA aneurysms. Dotted line is dural incision. ICA : internal carotid artery, ACoA : anterior communicating artery.
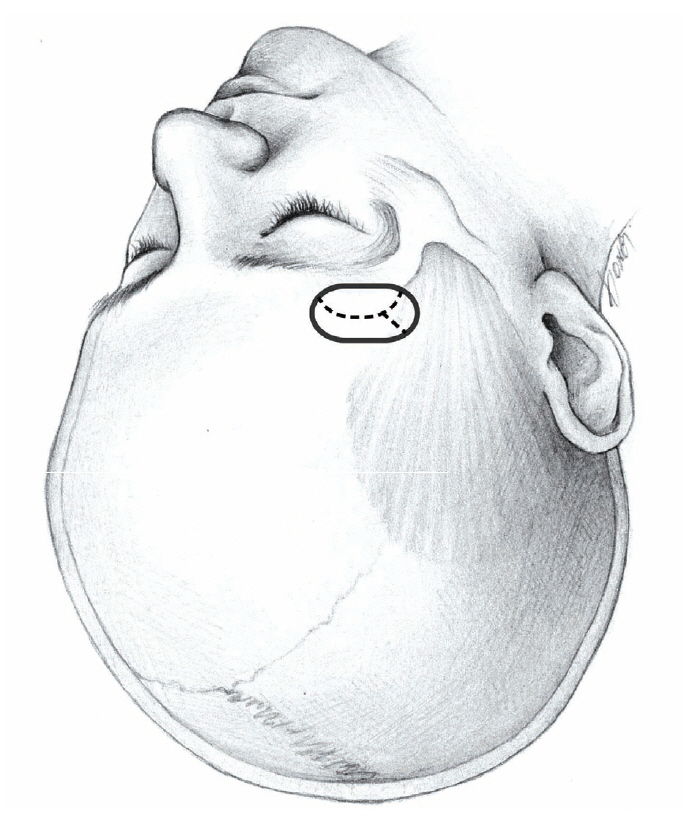
Fig. 2. Cranial opening for MCA aneurysms. Dotted line is dural incision. MCA : middle cerebral artery.
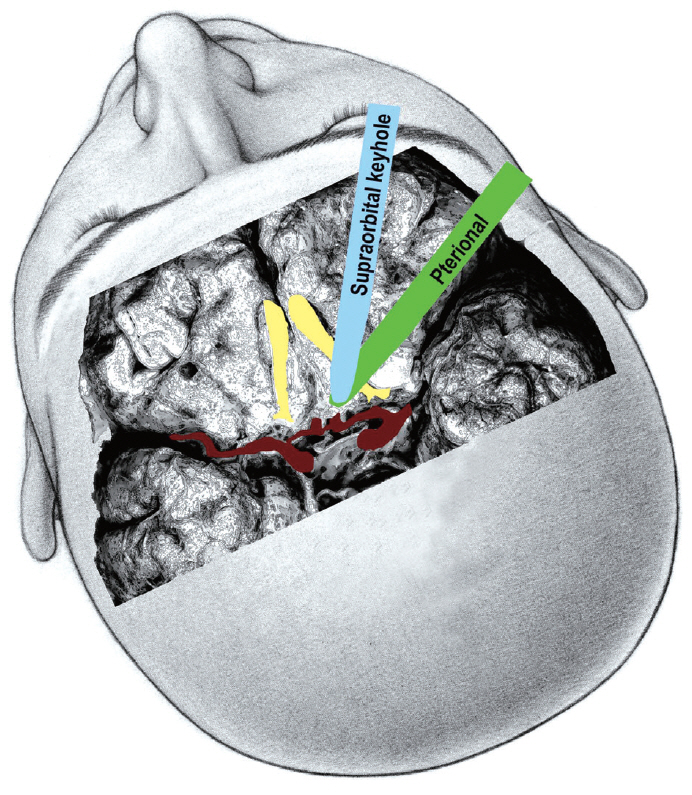
Fig. 3. Location of the brain spatula applied to the inferior surface of the frontal lobes in a supraorbital keyhole approach and pterional approach for ACoA aneurysms. ACoA : anterior communicating artery.
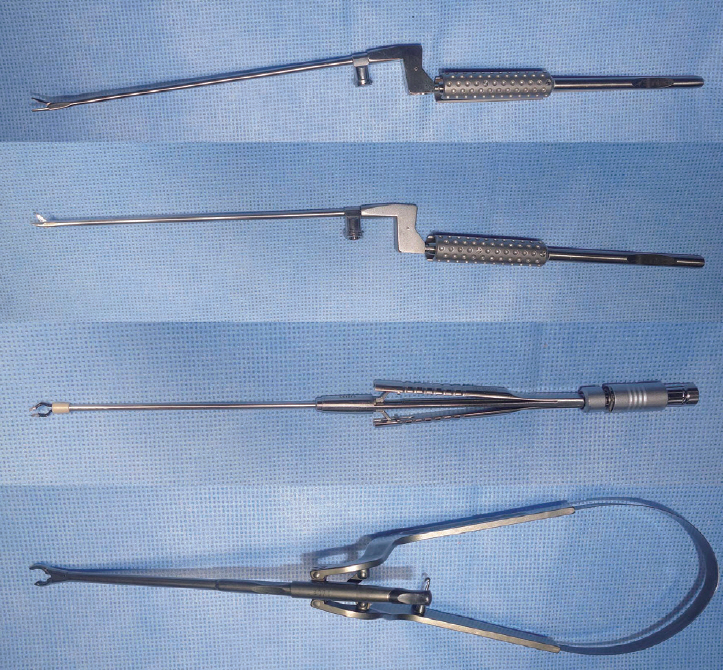
Fig. 4. Single-shaft slender-type surgical instruments, including microforceps, microscissors, bipolar coagulator, and aneurysm clip applier.
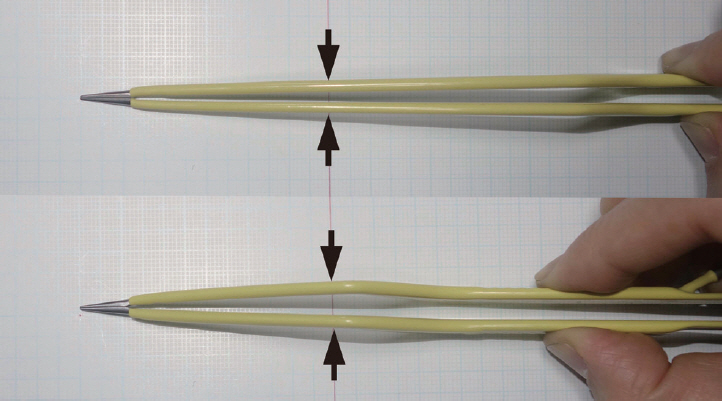
Fig. 5. Long and short bipolar coagulation forceps. The long bipolar coagulation forceps have a narrower configuration in the anterior part. Arrows indicate the width of the bipolar coagulation forceps at the level of the craniotomy opening.
Cited by 2 articles
-
Keyhole approach in anterior circulation aneurysm: Current indication, advantages, technical limitations, complications and their avoidance
Hanuman Prajapati, Ahmad Ansari, Manish Jaiswal
J Cerebrovasc Endovasc Neurosurg. 2022;24(2):101-112. doi: 10.7461/jcen.2022.E2021.07.008.Effects of Scalp Nerve Block on the Quality of Recovery after Minicraniotomy for Clipping of Unruptured Intracranial Aneurysms : A Randomized Controlled Trial
Seungeun Choi, Young Hoon Choi, Hoo Seung Lee, Kyong Won Shin, Yoon Jung Kim, Hee-Pyoung Park, Won-Sang Cho, Hyongmin Oh
J Korean Neurosurg Soc. 2023;66(6):652-663. doi: 10.3340/jkns.2023.0010.
Reference
-
References
1. Brydon HL, Akil H, Ushewokunze S, Dhir JS, Taha A, Ahmed A. Supraorbital microcraniotomy for acute aneurysmal subarachnoid haemorrhage: results of first 50 cases. Br J Neurosurg. 22:40–45. 2008.
Article2. Cardali S, Romano A, Angileri FF, Conti A, La Torre D, de Divitiis O, et al. Microsurgical anatomic features of the olfactory nerve: relevance to olfaction preservation in the pterional approach. Neurosurgery. 57(1 Suppl):17–21. 2005.
Article3. Chalouhi N, Jabbour P, Ibrahim I, Starke RM, Younes P, El Hage G, et al. Surgical treatment of ruptured anterior circulation aneurysms: comparison of pterional and supraorbital keyhole approaches. Neurosurgery. 72:437–441. 2013.4. Chen L, Tian X, Zhang J, Huang Y, Chen E, Lan Q. Is eyebrow approach suitable for ruptured anterior circulation aneurysms on early stage: a prospective study at a single institute. Acta Neurochir (Wien). 151:781–784. 2009.
Article5. Choi YJ, Son W, Park KS, Park J. Intradural procedural time to assess technical difficulty of superciliary keyhole and pterional approaches for unruptured middle cerebral artery aneurysms. J Korean Neurosurg Soc. 59:564–569. 2016.
Article6. Goh DH, Kim GJ, Park J. Medpor craniotomy gap wedge designed to fill small bone defects along cranial bone flap. J Korean Neurosurg Soc. 46:195–198. 2009.
Article7. Lan Q, Gong Z, Kang D, Zhang H, Qian Z, Chen J, et al. Microsurgical experience with keyhole operations on intracranial aneurysms. Surg Neurol. 66 Suppl 1:S2–S9. 2006.
Article8. Lan Q, Zhang H, Zhu Q, Chen A, Chen Y, Xu L, et al. Keyhole approach for clipping intracranial aneurysm: comparison of supraorbital and pterional keyhole approach. World Neurosurg. 102:350–359. 2017.
Article9. Lee YS, Park J. Anterior choroidal artery aneurysm surgery: ischemic complications and clinical outcomes revisited. J Korean Neurosurg Soc. 54:86–92. 2013.
Article10. Mitchell P, Vindlacheruvu RR, Mahmood K, Ashpole RD, Grivas A, Mendelow AD. Supraorbital eyebrow minicraniotomy for anterior circulation aneurysms. Surg Neurol. 63:47–51. 2005.
Article11. Mori K, Wada K, Otani N, Tomiyama A, Toyooka T, Takeuchi S, et al. Keyhole strategy aiming at minimizing hospital stay for surgical clipping of unruptured middle cerebral artery aneurysms. J Neurosurg. 130:1039–1408. 2019.
Article12. Paladino J, Mrak G, Miklic P, Jednacak H, Mihaljevic D. The keyhole concept in aneurysm surgery--a comparative study: keyhole versus standard craniotomy. Minim Invasive Neurosurg. 48:251–258. 2005.
Article13. Park HS, Park SK, Han YM. Microsurgical experience with supraorbital keyhole operations on anterior circulation aneurysms. J Korean Neurosurg Soc. 46:103–108. 2009.
Article14. Park J. Self-drilling anchor screws for dural tenting sutures: technical note. Surg Neurol. 72:175–176. 2009.15. Park J. Superciliary keyhole approach for unruptured anterior circulation aneurysms: surgical technique, indications, and contraindications. J Korean Neurosurg Soc. 56:371–374. 2014.
Article16. Park J. Clip-knotting technique for intracranial arterial suturing through deep and narrow surgical corridors-how I do it. Acta Neurochir (Wien). 157:769–771. 2015.
Article17. Park J, Hwang YH, Huh S, Kang DH, Kim Y. Minimally invasive and rapid surgical embolectomy (MIRSE) as rescue treatment following failed endovascular recanalization for acute ischemic stroke. Acta Neurochir (Wien). 156:2041–2049. 2014.
Article18. Park J, Hwang YH, Kim Y. Extended superciliary approach for middle cerebral artery embolectomy after unsuccessful endovascular recanalization therapy: technical note. Neurosurgery. 65:E1191–E1194. 2009.19. Park J, Jung TD, Kang DH, Lee SH. Preoperative percutaneous mapping of the frontal branch of the facial nerve to assess the risk of frontalis muscle palsy after a supraorbital keyhole approach. J Neurosurg. 118:1114–1119. 2013.
Article20. Park J, Kang DH, Chun BY. Superciliary keyhole surgery for unruptured posterior communicating artery aneurysms with oculomotor nerve palsy: maximizing symptomatic resolution and minimizing surgical invasiveness. J Neurosurg. 115:700–706. 2011.
Article21. Park J, Son W, Kwak Y, Ohk B. Pterional versus superciliary keyhole approach: direct comparison of approach-related complaints and satisfaction in the same patient. J Neurosurg. 130:220–226. 2018.
Article22. Park J, Woo H, Kang DH, Sung JK, Kim Y. Superciliary keyhole approach for small unruptured aneurysms in anterior cerebral circulation. Neurosurgery. 68(2 Suppl Operative):300–309. 2011.
Article23. Park JS, Kim H, Baik MW, Park IS. Risk factor analysis for poor outcomes in supraorbital keyhole aneurysm clipping for ruptured anterior circulation aneurysms. World Neurosurg. 111:e386–e394. 2018.
Article24. Pitanguy I, Ramos AS. The frontal branch of the facial nerve: the importance of its variations in face lifting. Plast Reconstr Surg. 38:352–356. 1966.25. Raaymakers TW, Rinkel GJ, Limburg M, Algra A. Mortality and morbidity of surgery for unruptured intracranial aneurysms: a meta-analysis. Stroke. 29:1531–1538. 1998.
Article26. Ramos-Zúñiga R, Velázquez H, Barajas MA, López R, Sánchez E, Trejo S. Trans-supraorbital approach to supratentorial aneurysms. Neurosurgery. 51:125–130. 2002.
Article27. Reisch R, Marcus HJ, Kockro RA, Ulrich NH. The supraorbital keyhole approach: how I do it. Acta Neurochir (Wien). 157:979–983. 2015.
Article28. Reisch R, Perneczky A. Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery. 57(4 Suppl):242–255. 2005.
Article29. Rychen J, Croci D, Roethlisberger M, Nossek E, Potts M, Radovanovic I, et al. Minimally invasive alternative approaches to pterional craniotomy: a systematic review of the literature. World Neurosurg. 113:163–179. 2018.
Article30. Shin D, Park J. Unruptured supraclinoid internal carotid artery aneurysm surgery: superciliary keyhole approach versus pterional approach. J Korean Neurosurg Soc. 52:306–311. 2012.
Article31. Tomii M. Strength testing of the human olfactory nerve at the frontal skull base. Neurosurg Rev. 35:555–560. 2012.
Article32. Tra H, Huynh T, Nguyen B. Minipterional and supraorbital keyhole craniotomies for ruptured anterior circulation aneurysms: experience at single center. World Neurosurg. 109:36–39. 2018.
Article33. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms: concept and technique. Surg Neurol. 49:481–489. 1998.
Article34. Yu LB, Huang Z, Ren ZG, Shao JS, Zhang Y, Wang R, et al. Supraorbital keyhole versus pterional craniotomies for ruptured anterior communicating artery aneurysms: a propensity score-matched analysis. Neurosurg Rev. 2018; [Epub ahead of print].
Article35. Zumofen DW, Rychen J, Roethlisberger M, Taub E, Kalbermatten D, Nossek E, et al. A review of the literature on the transciliary supraorbital keyhole approach. World Neurosurg. 98:614–624. 2017.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microsurgical Experience with Supraorbital Keyhole Operations on Anterior Circulation Aneurysms
- Modified Supraorbital Keyhole Approach to Anterior Circulation Aneurysms
- Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
- Comparison between Lateral Supraorbital Approach and Pterional Approach in the Surgical Treatment of Unruptured Intracranial Aneurysms
