Pterional-subolfactory Approach for Treatment of High Positioned Anterior Communicating Artery Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, and Chonnam National University Research Institute of Medical Sciences, Chonnam National University Hwasun Hospital & Medical School, Gwangju, Korea. taesun1963@yahoo.co.kr
- KMID: 1491436
- DOI: http://doi.org/10.7461/jcen.2013.15.3.177
Abstract
OBJECTIVE
The purpose of this study is to compare the surgical outcomes of pterional-subolfactory approach for the high positioned anterior communicating artery (ACoA) aneurysm with the conventional pterional approach.
METHODS
Between February 2005 and December 2012, 463 ACoA aneurysms were surgically treated in our institution. Forty eight high positioned ACoA aneurysms were treated with pterional-subolfactory or conventional pterional approach. High positioned ACoA aneurysms were defined as aneurysms located higher than 10 mm above the anterior clinoid process. Pterional-subolfactory approach is a procedure including dissection of olfactory tract and resection of the gyrus rectus inferior and medial to the olfactory tract. Thirty-four of the 48 cases were treated with pterional-subolfactory approach and 14 were treated conventionally.
RESULTS
There were 2 postoperative cerebral infarction with the conventional pterional approach, but none with the pterional-subolfactory approach group (p = 0.026). Postoperative digital subtraction angiography revealed significant remnant aneurysm in the conventional pterional approach group. All patients with unruptured aneurysms had good clinical outcomes with Glasgow outcome score of 5. Among ruptured ACoA aneurysm patients, 2 patients with conventional pterional approach had postoperative cerebral infarctions but permanent neurologic deficit was found in only 1 patient. Three patients treated with the pterional-subolfactory approach, who had preoperative ruptured aneurysms had poor clinical outcomes. The mean operation time for the conventional pterional approach was 58 minutes longer than for the pterional-subolfactory approach (p = 0.001).
CONCLUSION
We concluded that pterional-subolfactory approach is highly preferable for cases of high positioned ACoA aneurysm, giving a wide and effective operation view.
MeSH Terms
Figure
-
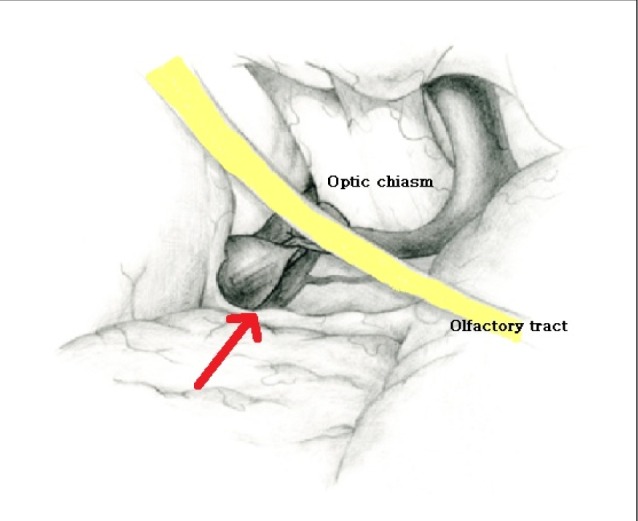
Fig. 1 Schematic drawing of subolfactory approach; dissection of olfactory tract and suck out of rectus gyrus inferomedial of olfactory tract allows no need for retractor and direct visualization of high-positioned anterior communicating artery aneurysm (Arrow: direction of approach).
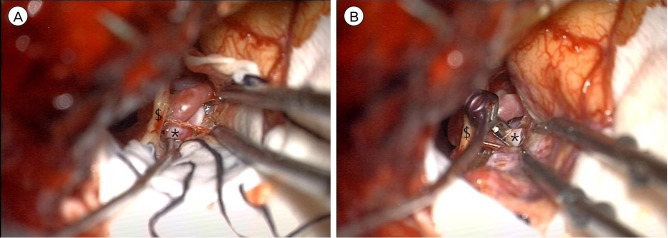
Fig. 2 (A) Operative photo of subolfactory approach: direct visualization of high-positioned anterior communicating artery aneurysm with minimal retraction with no retractor. (B) Operative photo of subolfactory approach: direct visualization of high-positioned anterior communicating artery aneurysm with minimal retraction with no retractor (clipped state). $: olfactory nerve, *: anterior communicating artery aneurysm.
Cited by 1 articles
-
Postoperative Clipping Status after a Pterional versus Interhemispheric Approach for High-Positioned Anterior Communicating Artery Aneurysms
Myungsoo Kim, Byoung-Joon Kim, Wonsoo Son, Jaechan Park
J Korean Neurosurg Soc. 2021;64(4):524-533. doi: 10.3340/jkns.2020.0215.
Reference
-
1. Fujiwara H, Yasui N, Nathal-Vera E, Suzuki A. Anosmia after anterior communicating artery aneurysm surgery: Comparison between the anterior interhemispheric and basal interhemispheric approaches. Neurosurgery. 1996; 2. 38(2):325–328. PMID: 8869060.
Article2. Horikoshi T, Nukui H, Mitsuka S, Kaneko M. Partial resection of the gyrus rectus in pterional approach to anterior communicating artery aneurysms. Neurol Med Chir (Tokyo). 1992; 3. 32(3):136–139. PMID: 1377795.
Article3. Kempe LG, VanderArk GD. Anterior communicating artery aneurysms. Gyrus rectus approach. Neurochirurgia (Stuttg). 1971; 3. 14(2):63–70. PMID: 5555315.
Article4. Locksley HB. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. Based on 6368 cases in the cooperative study. J Neurosurg. 1966; 8. 25(2):219–239. PMID: 5911370.5. Norlen G, Barnum AS. Surgical treatment of aneurysms of the anterior communicating artery. J Neurosurg. 1953; 11. 10(6):634–650. PMID: 13109559.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interhemispheric Approach for Intracranial Aneurysms
- Postoperative Clipping Status after a Pterional versus Interhemispheric Approach for High-Positioned Anterior Communicating Artery Aneurysms
- The Optimal Surgical Direction Concerning the Pterional Approach to the Anterior Communicating Artery Aneurysms
- Surgical Treatment of Anterior Communicating Artery Aneurysms
- Analysis on the Early Surgical Results of Patients with Poor-grade Anterior Communicating Artery Aneurysms via Frontotemporal-transorbital Approach
