A Case of Cushing's Disease with Renal Cell Carcinomaand End-stage Renal Disease
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea, College of Medicine, Korea.
- KMID: 2178244
- DOI: http://doi.org/10.3803/jkes.2007.22.1.62
Abstract
- Cushing's disease is the most common cause of endogenous Cushing's syndrome caused by the excessive secretion of adrenocorticotropic hormone (ACTH) by pituitary ACTH-secreting tumors. The tumors are usually microadenomas (< 10 mm in diameter). Macroadenomas are rare, and corticotroph hyperplasia and carcinomas are extremely rare. Patients with these tumors exhibit an increase in plasma ACTH and cortisol levels, elevated urinary excretion of cortisol and adrenocortical steroid metabolites, evidence of altered negative feedback of cortisol and disturbances in neuroendocrine regulation. The diagnosis of Cushing's disease can be challenging in patients with renal failure the presence of abnormal plasma cortisol, poor gastrointestinal tract absorption of dexamethasone and altered functioning of the hypophyseal-pituitary-adrenal axis have been reported in end-stage renal disease, and the urinary cortisol increment method is not reliable in these patients. The prevalence of renal cell carcinoma in patients on dialysis is higher than in the general population. We recently treated a patient with Cushing's disease and end-stage renal disease as a result of renal cell carcinoma. The diagnosis was made by laboratory evaluation of plasma and radiological examination. Here we report a case of Cushing's disease with a review of the medical literature.
MeSH Terms
-
Absorption
Adrenocorticotropic Hormone
Axis, Cervical Vertebra
Carcinoma, Renal Cell
Corticotrophs
Cushing Syndrome
Dexamethasone
Diagnosis
Dialysis
Gastrointestinal Tract
Humans
Hydrocortisone
Hyperplasia
Kidney Failure, Chronic*
Plasma
Prevalence
Renal Insufficiency
Adrenocorticotropic Hormone
Dexamethasone
Hydrocortisone
Figure
-

Fig. 1 Central obesity, moon face (A) and abdominal purple striae (B) in 38 years old women with Cushing's disease.
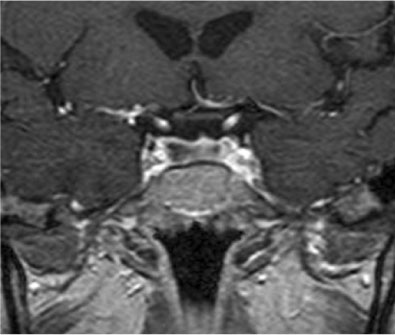
Fig. 2 Coronal section of sellar MRI scan shows l.5 cm sized pituitary mass with a left deviated pituitary stalk. T2 weighted enhanced coronal section image.
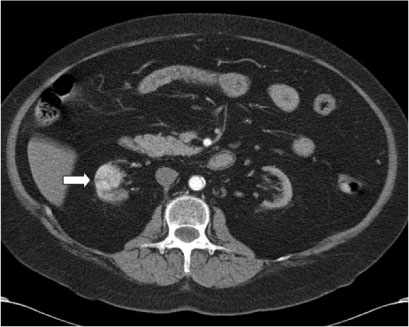
Fig. 3 Abdmonen CT shows a 2.9 × 2.5 × 2.3 cm sized enhancing mass in the right kidney.

Fig. 4 Histology of the pituitary mass. A. Tumor cells have eosinophilic cytoplasm and relatively uniform, polygonal cells arrayed in cords. (H&E stain, ×400) B. Immunohistochemial stain of pituitary adenoma shows diffuse and strongly reactive with ACTH (adrenocorticotropic hormone). (IHC, ×400)

Fig. 5 Histological examination of the right kidney shows well differentiated tumor cell with abundant clear cytoplasm. (H&E stain, ×200)
Reference
-
1. Cushing WH. The basophilic adenomas of the pituitary body and their clinical manifestations. Bull Johns Hopkin's Hospital. 1932. 50:137–195.2. Howlett TA, Ress LH, Besser GM. Cushing's syndrome. Clinics Endocrinol Metab. 1985. 14:911–913.3. Carpenter PC. Cushing syndrome: Update of diagnosis and management. Mayo Clin Proc. 1986. 61:49–51.4. Ramirez G, Gomez-Sanchez C, Meikle AW, Jubiz W. Evaluation of the hypothalamic hypophyseal adrenal axis in patients receiving long-term hemodialysis. Arch Intern Med. 1982. 142:1448–1452.5. Sharp NA, Devlin JT, Rimmer JM. Renal failure obfuscates the diagnosis of Cushing's disease. JAMA. 1986. 256:2564–2565.6. Ishikawa I. Renal cell carcinoma in chronic hemodialysis pateints- A 1990 questionnaire study in Japan. Kidney Int Suppl. 1993. 41:S167–S169.7. Cook DM, Louriax DL. Cushing's syndorme. Curr Ther Endocrinol Metab. 1994. 5:142–146.8. Orth DN. Cushing's syndrome. N Engl J Med. 1995. 332:791–801.9. Newell-Price J, Tainer P, Besser M, Grossman A. The diagnosis and differential diagnosis of Cushing's syndrome and pseudo-Cushing's states. Endocr Rev. 1998. 19:647–672.10. The Korean society of endocrinology, The committee for endocrine disease in Korea. The incidence and clinical characteristics of Cushing's syndrome in Korea. J Kor Soc Endocrinol. 2000. 15:31–45.11. Oguz Y, Oktenli C, Ozata M, Ozgurtas T, Sanisoglu Y, Yenicesu M, Vural A. The midnight-to-morning urinary cortisol increment method is not reliable for the assessment of hypothalamic-pituitary-adrenal insufficiency in patients with end-stage kidney disease. J Endocrinol Invest. 2003. 26:609–615.12. Grant AC, Rodger RS, Mitchell R, Gibson S. Hypothalamio-pituitary-adrenal axis in uremia: evidence for primary adrenal dysfunction? Nephrol Dial Transplant. 1993. 8:307–310.13. Clodi M, Riedl M, Schmaldienst S, Vychytil A, Kotzmann H. Adrenal function in patients with chronic renal failure. Am J Kidney Dis. 1998. 32:52–55.14. Grossman AB, Howlett TA, Perry L, Coy DH, Savage MO, Lavender L, Ress LH, Besser GM. CRF in the differential diagnosis of Cushing's syndrome: a comparison with the dexamethasone suppression test. Clin Endocrinol. 1988. 29:167–178.15. Otokida K, Fujiwara T, Oriso S, Kato M. Cortisol and its metabolites in the plasma and urine in Cushing's syndrome with chronic renal failure(CRF), compared to Cushing's syndrome without CRF. Nippon Jinzo Gakkai Shi. 1989. 31:651–656.16. Oldfield EH, Doppman JL, Nieman LK, Chrousos GP, Miller DL, Katz DA, Cutler GB, Loriaux DL. Petrosal sinus sampling with and without corticotropin-releasing hormone for the differential diagnosis of Cushing's syndrome. N Engl J Med. 1991. 325:897–905.17. de Herder W, Uitterlinden P, Pieterman H, Tanghe HL, Kwekkeboom DJ, Pols HA, van de Berge JH, Lamberts SW. Pituitary tumor localization in patients with Cushing's disease by magnetic resonance imaging: Is there a place for petrosal sinus sampling? Clin Endocrinol. 1994. 40:87–92.18. Mampalam TJ, Tyrell JB, Wilson CB. Trans-sphenoidal microsurgery for Cushing's disease. A report of 216 cases. Ann Intern Med. 1998. 109:487–493.19. Adachi M, Takayanagi R, Yanase T, Sakai Y, Ikuyama S, Nakagaki H, Osamura Y, Sanno N, Nawata H. Cyclic Cushing's disease in long-term remission with a daily low dose of bromocriptine. Intern Med. 1996. 35:207–211.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acquired Cystic Kidney Disease in Patients Undergoing Long-term Hemodialysis Treatment
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- Renal Cell Carcinoma in Patients on Dialysis for End-Stage Renal Disease
- Leukemoid reaction with renal cell carcinoma
- Letter to the Editor: Is Routine Screening Necessary for Renal Cell Carcinoma in End-Stage Renal Disease Patients?
