Ewha Med J.
2014 Sep;37(2):131-135. 10.12771/emj.2014.37.2.131.
Portal Vein Thrombosis in Minimal Change Disease
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. hansh@yuhs.ac
- KMID: 2171297
- DOI: http://doi.org/10.12771/emj.2014.37.2.131
Abstract
- Among the possible venous thromboembolic events in nephrotic syndrome, renal vein thrombosis and pulmonary embolism are common, while portal vein thrombosis (PVT) is rare. This report describes a 26-year-old man with histologically proven minimal change disease (MCD) complicated by PVT. The patient presented with epigastric pain and edema. He had been diagnosed with MCD five months earlier and achieved complete remission with corticosteroids, which were discontinued one month before the visit. Full-blown relapsing nephrotic syndrome was evident on laboratory and clinical findings, and an abdominal computed tomography revealed PVT. He immediately received immunosuppressants and anticoagulation therapy. An eight-week treatment resulted in complete remission, and a follow-up abdominal ultrasonography showed disappearance of PVT. In conclusion, PVT is rare and may not be easily diagnosed in patients with nephrotic syndrome suffering from abdominal pain. Early recognition of this rare complication and prompt immunosuppression and anticoagulation therapy are encouraged to avoid a fatal outcome.
MeSH Terms
-
Abdominal Pain
Adrenal Cortex Hormones
Adult
Anticoagulants
Edema
Fatal Outcome
Follow-Up Studies
Humans
Immunosuppression
Immunosuppressive Agents
Nephrosis, Lipoid*
Nephrotic Syndrome
Proteinuria
Pulmonary Embolism
Renal Veins
Thrombosis
Ultrasonography
Venous Thrombosis*
Adrenal Cortex Hormones
Anticoagulants
Immunosuppressive Agents
Figure
-
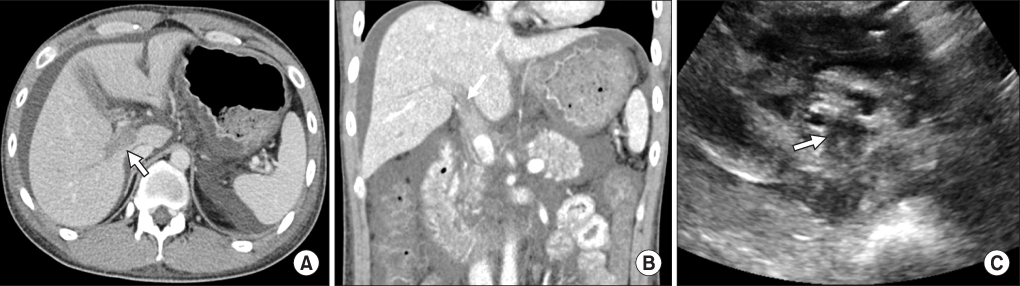
Fig. 1 Imaging studies for portal vein thrombosis. (A) Transverse and (B) coronal views of an abdominal computed tomography scan clearly show portal vein thrombosis (arrow). (C) Thrombi are also noted in an abdominal ultrasonography (arrow).

Fig. 2 Follow-up abdominal ultrasonography eight weeks after the onset of portal vein thrombosis. There is no evidence of thrombi in portal vein, suggesting resolution of portal vein thrombosis after complete remission was achieved.
Reference
-
1. Kerlin BA, Ayoob R, Smoyer WE. Epidemiology and pathophysiology of nephrotic syndrome-associated thromboembolic disease. Clin J Am Soc Nephrol. 2012; 7:513–520.2. Singhal R, Brimble KS. Thromboembolic complications in the nephrotic syndrome: pathophysiology and clinical management. Thromb Res. 2006; 118:397–407.3. Glassock RJ. Prophylactic anticoagulation in nephrotic syndrome: a clinical conundrum. J Am Soc Nephrol. 2007; 18:2221–2225.4. Loscalzo J. Venous thrombosis in the nephrotic syndrome. N Engl J Med. 2013; 368:956–958.5. Ozsoylu S, Strauss HS, Diamond LK. Effects of corticosteroids on coagulation of the blood. Nature. 1962; 195:1214–1215.6. Bostom AG, Shemin D. Abnormalities of lipoprotein metabolism in the nephrotic syndrome. N Engl J Med. 1991; 324:697–698.7. Fahal IH, McClelland P, Hay CR, Bell GM. Arterial thrombosis in the nephrotic syndrome. Postgrad Med J. 1994; 70:905–909.8. Woolf AS, Street PR, Walmsley KM, Cohen SL. Portal vein thrombosis in the nephrotic syndrome. Nephrol Dial Transplant. 1989; 4:581–582.9. De Luca M, Dugo M, Arduini R, Liessi G. Acute venous thrombosis of spleno-mesenteric portal axis: an unusual localization of thromboembolism in the nephrotic syndrome. Am J Nephrol. 1991; 11:260–263.10. Plaisier EM, Legallicier B, Faintuch JM, Ronco PM. Acute portal vein thrombosis at the onset of a nephrotic syndrome. Nephrol Dial Transplant. 1996; 11:696–698.11. Etoh Y, Ohsawa I, Fujita T, Fuke Y, Endo M, Ohi H, et al. Nephrotic syndrome with portal, splenic and renal vein thrombosis. A case report. Nephron. 2002; 92:680–684.12. Varghese J, Mathew A, Seethalekshmy NV, Kurian G, Unni VN. Isolated portal vein thrombosis in nephrotic syndrome. Indian J Nephrol. 2007; 17:26–28.13. Sun L, Xu C. Portal vein thrombosis as the first sign of nephrotic syndrome. Nat Clin Pract Nephrol. 2008; 4:342–345.14. Bian F, Ge QM, Jiang GR, Wen LP. Cavernous transformation of the portal vein in nephrotic syndrome. Vasa. 2011; 40:323–326.15. Wang YC, Chuang FR, Lee WC, Chen TC, Ko SF, Wang IK, et al. Low-molecular-weight heparin successfully used to treat a nephrotic patient complicated by superior mesenteric vein thrombosis and portal vein thrombosis. Med Princ Pract. 2011; 20:196–199.16. Wang J, Fan Q, Chen Y, Dong X, Zhang Y, Feng J, et al. A case report of minimal change nephrotic syndrome complicated with portal, splenic and superior mesenteric vein thrombosis. Clin Nephrol. 2012; 77:505–509.17. Sogaard KK, Astrup LB, Vilstrup H, Gronbaek H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol. 2007; 7:34.18. Turnes J, Garcia-Pagan JC, Gonzalez M, Aracil C, Calleja JL, Ripoll C, et al. Portal hypertension-related complications after acute portal vein thrombosis: impact of early anticoagulation. Clin Gastroenterol Hepatol. 2008; 6:1412–1417.19. Condat B, Pessione F, Helene Denninger M, Hillaire S, Valla D. Recent portal or mesenteric venous thrombosis: increased recognition and frequent recanalization on anticoagulant therapy. Hepatology. 2000; 32:466–470.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Steroid Resistant Minimal Change Disease Associated with Portal Vein Thrombosis Treated by Combined Immunosuppressive Agents
- A Case of Minimal Change Nephrotic Syndrome Presented as Portal Vein Thrombosis and Acute Renal Failure
- Radiologic Findings of Neonatal Cerebral Infarction related with Portal Vein Thrombosis: Case Report
- Acute Appendicitis with Superior Mesenteric Vein Thrombosis and Portal Vein Thrombosis
- Portal Vein Thrombosis during Pregnancy
