Electrolyte Blood Press.
2012 Dec;10(1):18-25. 10.5049/EBP.2012.10.1.18.
Etiology of Hypokalemic Paralysis in Korea: Data from a Single Center
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Kyung Hee University, Seoul, Korea. wonkid@chollian.net
- KMID: 2168390
- DOI: http://doi.org/10.5049/EBP.2012.10.1.18
Abstract
- Recognizing the underlying causes of hypokalemic paralysis seems to be essential for the appropriate management of affected patients and their prevention of recurrent attacks. There is, however, a paucity of documented reports on the etiology of hypokalemic paralysis in Korea. We retrospectively analyzed 34 patients with acute flaccid weakness due to hypokalaemia who were admitted during the 5-year study period in order to determine the spectrum of hypokalemic paralysis in Korea and to identify the differences in clinical parameters all across the causes of hypokalemic paralysis. We divided those 34 patients into 3 groups; the 1st group, idiopathic hypokalemic periodic paralysis (HPP), the 2nd, thyrotoxic periodic paralysis (TPP), and the 3rd group, secondary hypokalemic paralysis (HP) without TPP. Seven of the patients (20.6%) were diagnosed as idiopathic HPP considered the sporadic form, and 27 patients (79.4%) as secondary HP. Among the patients diagnosed as secondary HP, 16 patients (47.1%) had TPP. Patients of secondary hypokalemic paralysis without TPP required a longer recovery time compared with those who had either idiopathic HPP or TPP. This is due to the fact that patients of secondary HP had a significantly negative total body potassium balance, whereas idiopathic HPP and TPP were only associated with intracellular shift of potassium. Most of the TPP patients included in our study had overt thyrotoxicosis while 3 patients had subclinical thyrotoxicosis. This study shows that TPP is the most common cause of hypokalemic paralysis in Korea. And we suggest that doctors should consider the presence of TPP in patients of hypokalemic paralysis even if they clinically appear to be euthyroid state.
MeSH Terms
Figure
-

Fig. 1 Etiology of hypokalemic paralysis from a single center in Korea for 5 years. HPP, hypokalemic periodic paralysis; TPP, thyrotoxic periodic paralysis; dRTA, distal renal tubular acidosis.
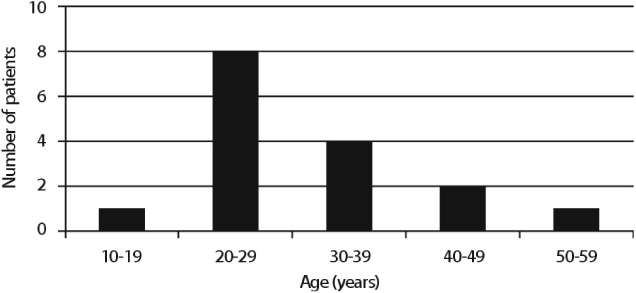
Fig. 2 Age distribution of thyrotoxic periodic paralysis.
Cited by 1 articles
-
Thyrotoxic hypokalemic periodic paralysis due to Graves’ disease in 2 adolescents
Jung Gi Roh, Kyu Jung Park, Hae Sang Lee, Jin Soon Hwang
Ann Pediatr Endocrinol Metab. 2019;24(2):133-136. doi: 10.6065/apem.2019.24.2.133.
Reference
-
1. Ahlawat SK, Sachdev A. Hypokalemic paralysis. Postgrad Med J. 1999. 75:193–197.2. Kalita J, Nair PP, Kumar G, et al. Renal tubular acidosis presenting as respiratory paralysis: Report of a case and review of literature. Neurol India. 2010. 58:106–108.
Article3. Stedwell RE, Allen KM, Binder LS. Hypokalemic paralyses: a review of the etiologies, pathophysiology, presentation, and therapy. Am J Emerg Med. 1992. 10:143–148.
Article4. Lin SH, Lin YF, Halperin ML. Hypokalemia and paralysis. Q J Med. 2001. 94:133–139.5. Ko GTC, Chow CC, Yeung VTF, Chan HHL, Li JKY, Cockram CS. Thyrotoxic periodic paralysis in a Chinese population. Q J Med. 1996. 89:463–468.
Article6. Ober KP. Thyrotoxic periodic paralysis in the United States. Report of 7 cases and review of the literature. Medicine (Baltimore). 1992. 71:109–120.
Article7. Sinharay R. Hypokalaemic thyrotoxic periodic paralysis in an Asian man in the United Kingdom. Emerg Med J. 2004. 21:120–121.
Article8. Sternberg D, Maisonobe T, Jurkat-Rott K, et al. Hypokalemic periodic paralysis type 2 caused by mutations at codon 672 in the muscle sodium channel gene SCN4A. Brain. 2001. 124:1091–1099.
Article9. Fontaine B, Vele-Santos JM, Jurkat-Rott K, et al. Mapping of hypokalemic periodic paralysis locus to chromosome 1q31-q32 in three European families. Nat Genet. 1994. 6:267–272.
Article10. Grosson CL, Esteban J, Mckenna-Yasek D, Gusella JF, et al. Hypokalemic periodic paralysis mutations: confirmation of mutation and analysis of founder effect. Neuromuscul Disord. 1996. 6:27–31.
Article11. Fouad G, Dalakas M, Servidei S, et al. Genotype-phenotype correlations of DHP receptor alpha 1-subunit gene mutations causing hypokalemic periodic paralysis. Neuromusc Disord. 1997. 7:33–38.
Article12. Jurkat-Rott K, Mitrovic N, Hang C, et al. Voltage-sensor sodium channel mutations cause hypokalemic periodic paralysis type 2 by enhanced inactivation and reduced current. Proc Natl Acad Sci USA. 2000. 97:9549–9554.
Article13. Lin SH, Chiu JS, Hsu CW, et al. A simple and rapid approach to hypokalemic paralysis. Am J Emerg Med. 2003. 21:487–491.
Article14. Maurya PK, Kalita J, Misra UK. Spectrum of hypokalaemic periodic paralysis in a tertiary care centre in India. Postgrad Med J. 2010. 86:692–695.
Article15. Miyashita Y, Monden T, Yamamoto K, et al. Ventricular fibrillation due to severe hypokalemia induced by steroid treatment in a patient with thyrotoxic periodic paralysis. Intern Med. 2006. 45:11–13.
Article16. Lin SH, et al. Thyrotoxic periodic paralysis. Mayo Clin Proc. 2005. 80:99–105.
Article17. Kung AW. Clinical review: thyrotoxic periodic paralysis: a diagnostic challenge. J Clin Endocrinol Metab. 2006. 91:2490–2495.18. McFadzean AJ, Yeung R. Periodic paralysis complicating thyrotoxicosis in Chinese. Br Med J. 1967. 1:451–455.
Article19. Gordon GG, Southren AL. Thyroid-hormone effects on steroid-hormone metabolism. Bull N Y Acad Med. 1977. 53:241–259.20. Olivo J, Gordon GG, Rafii F, et al. Estrogen metabolism in hyperthyroidism and in cirrhosis of the liver. Steroids. 1975. 26:47–56.
Article21. Deenadayalu VP, White RE, Stallone JN, et al. Testosterone relaxes coronary arteries by opening the largeconductance, calciumactivated potassium channel. Am J Physiol Heart Circ Physiol. 2001. 281:H1720–H1727.
Article22. White RE, Han G, Maunz M, et al. Endotheliumindependent effect of estrogen on Ca(2+)-activated K(+) channels in human coronary artery smooth muscle cells. Cardiovasc Res. 2002. 53:650–661.
Article23. Manoukian MA, Foote JA, Crapo LM. Clinical and metabolic features of thyrotoxic periodic paralysis in 24 episodes. Arch Intern Med. 1999. 159:601–606.
Article24. Silva MR, Chiamolera MI, Kasamatsu TS, Cerutti JM, Maciel RM. Thyrotoxic hypokalemic periodic paralysis, an endocrine emergency: clinical and genetic features in 25 patients. Arq Bras Endocrinol Metabol. 2004. 48:196–215.25. Rone JK, Brietzke SA. Euthyroid thyrotoxic periodic paralysis. Mil Med. 1991. 156:434–436.
Article26. Coates JT, Mirick MJ, Rubino FJ. Thyrotoxic periodic paralysis with relapse during the euthyroid state. Wis Med J. 1987. 86:20–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypokalemic Paralysis: A Report of Two Different Cases
- A Case of Primary Sjiigren's Syndrome with Hypokalemic Paralysis and Renal Tubular Acidosis
- Persistent Hypokalemic Paralysis in a Patient with Graves’ Disease and Gitelman Syndrome
- Hypokalemic Periodic Paralysis
- Hypokalemic Periodic Paralysis Developed in a Patient with Neurogenic Diabetes Insipidus
