Ann Rehabil Med.
2014 Jun;38(3):401-404. 10.5535/arm.2014.38.3.401.
Arnold-Chiari Malformation Type III With Meningoencephalocele: A Case Report
- Affiliations
-
- 1Department of Physical and Rehabilitation Medicine, Inha University School of Medicine, Incheon, Korea. rmjung@inha.ac.kr
- 2Department of Physical and Rehabilitation Medicine, Inha University Hospital, Incheon, Korea.
- KMID: 2165760
- DOI: http://doi.org/10.5535/arm.2014.38.3.401
Abstract
- Arnold-Chiari malformation type III (CM III) is an extremely rare anomaly with poor prognosis. An encephalocele with brain anomalies as seen in CM II, and herniation of posterior fossa contents like the cerebellum are found in CM III. The female infant was a twin, born at 33 weeks, weighing 1.7 kg with a huge hydrocele on the craniocervical junction. After operations were performed, she was referred to the department of rehabilitation medicine for poor motor development, swallowing dysfunction, and poor eye fixation at 22 months. The child was managed with neurodevelopmental treatment, oromotor facilitation, and light perception training. After 14 months, improvement of gross motor function was observed, including more stable head control, rolling, and improvement of visual perception. CM III has been known as a condition with poor prognosis. However, with the improvement in operative techniques and intensive rehabilitations, the prognosis is more promising than ever before. Therefore, more attention must be paid to the rehabilitation issues concerning patients with CM III.
MeSH Terms
Figure
-
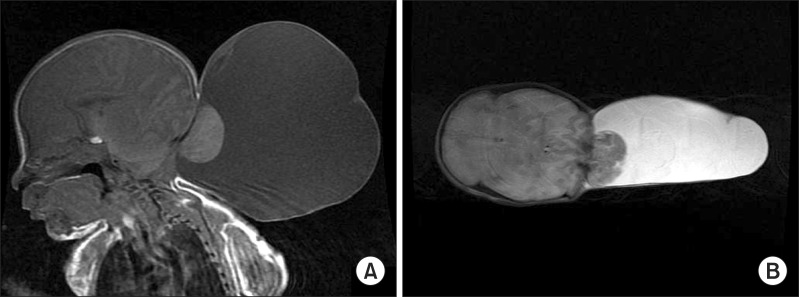
Fig. 1 (A) T1-weighted axial view and (B) T2-weighted sagittal view of brain magnetic resonance imaging at birth show a large sac with cerebellar herniation through the occipital area.
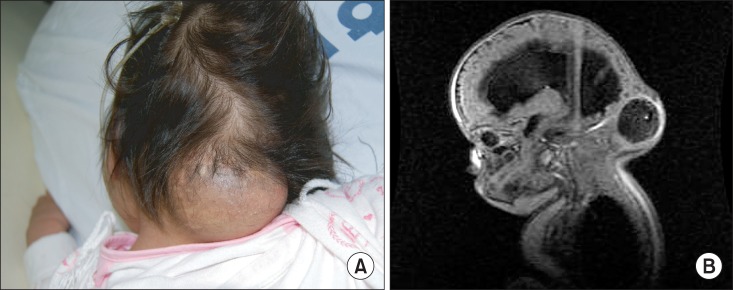
Fig. 2 (A) Photograph and (B) T1-weighted sagittal view of brain magnetic resonance imaging at 22 months show meningocele at the craniocervical junction with hydrocephalus after removal of the hydrocele.

Fig. 3 Visual perception training with penlight for cortical visual impairment in progress.
Reference
-
1. Chiari H. Concerning alterations in the cerebellum resulting from cerebral hydrocephalus. Pediatr Neurosci. 1987; 13:3–8. PMID: 3317333.2. Cama A, Tortori-Donati P, Piatelli GL, Fondelli MP, Andreussi L. Chiari complex in children: neuroradiological diagnosis, neurosurgical treatment and proposal of a new classification (312 cases). Eur J Pediatr Surg. 1995; 5(Suppl 1):35–38. PMID: 8770577.3. Castillo M, Quencer RM, Dominguez R. Chiari III malformation: imaging features. AJNR Am J Neuroradiol. 1992; 13:107–113. PMID: 1595427.4. Cho EY, Lee JJ, Lim JW, Choen EJ, Ko KO, Lee YH. A case of Chiari III malformation. J Korean Child Neurol Soc. 2005; 13:282–287.5. Hoyt CS. Visual function in the brain-damaged child. Eye (Lond). 2003; 17:369–384. PMID: 12724701.
Article6. Laget P, Flores-Guevara R, D'Allest AM, Ostre C, Raimbault J, Mariani J. Maturation of visually evoked potentials in the normal child. Electroencephalogr Clin Neurophysiol. 1977; 43:732–744. PMID: 72653.7. Dutton GN, Jacobson LK. Cerebral visual impairment in children. Semin Neonatol. 2001; 6:477–485. PMID: 12014888.
Article8. Malkowicz DE, Myers G, Leisman G. Rehabilitation of cortical visual impairment in children. Int J Neurosci. 2006; 116:1015–1033. PMID: 16861165.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of Arnold-Chiari malformation type II
- A case of Arnold-Chiari malformation
- Anesthetic management of a patient with Arnold-Chiari malformation type I with associated syringomyelia: A case report
- A Case of a Girl with Arnold-Chiari Type 1 Malformation with Precocious Puberty
- Arnold-Chiari Type I Malformation with Hemihypertrophy: A case report
