Prediction of Pathologic Grade and Prognosis in Mucoepidermoid Carcinoma of the Lung Using 18F-FDG PET/CT
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea. youngmog.shim@samsung.com
- 2Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- KMID: 2155569
- DOI: http://doi.org/10.3348/kjr.2015.16.4.929
Abstract
OBJECTIVE
The maximum standardized uptake value (SUVmax) of pulmonary mucoepidermoid carcinoma (PMEC) in fluorine-18fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) was evaluated as a preoperative predictor of pathologic grade and survival rate.
MATERIALS AND METHODS
Twenty-three patients who underwent preoperative PET/CT and complete resection for PMEC were enrolled. The optimal cut-off SUVmax for tumor grade was calculated as 6.5 by receiver operating characteristic curve. The patients were divided into a high SUV group (n = 7) and a low SUV group (n = 16). Clinicopathologic features were compared between the groups by chi2 test and overall survival was determined by Kaplan-Meier analysis.
RESULTS
The mean SUVmax was 15.4 +/- 11.5 in the high SUV group and 3.9 +/- 1.3 in the low SUV group. All patients except one from the low SUV group had low grade tumors and all had no nodal metastasis. The sensitivity and specificity of SUVmax from PET/CT for predicting tumor grade was 85.7% and 93.8%, respectively. During the follow-up period (mean, 48.6 +/- 38.7 months), four patients from the high SUV group experienced cancer recurrence, and one died of cancer. In contrast, none of the low SUV group had recurrence or mortality. Five-year overall survival rate was significantly higher in the low SUV group (100% vs. 71.4%, p = 0.031).
CONCLUSION
Pulmonary mucoepidermoid carcinoma patients with high SUVmax in PET/CT had higher tumor grade, more frequent lymph node metastasis and worse long-term outcome. Therefore, PMEC patients with high uptake on PET/CT imaging might require aggressive mediastinal lymph node dissection and adjuvant therapies.
MeSH Terms
-
Adolescent
Adult
Aged
Aged, 80 and over
Carcinoma, Mucoepidermoid/*pathology/radiography
Female
Fluorodeoxyglucose F18/metabolism
Humans
Kaplan-Meier Estimate
Lung Neoplasms/*pathology/radiography
Lymph Nodes/pathology/radiography
Lymphatic Metastasis
Male
Mediastinum/radiography
Middle Aged
Neoplasm Grading
Neoplasm Recurrence, Local/pathology/radiography
Positron-Emission Tomography/*methods
Prognosis
ROC Curve
Retrospective Studies
Sensitivity and Specificity
Survival Rate
Tomography, X-Ray Computed/*methods
Young Adult
Fluorodeoxyglucose F18
Figure
-
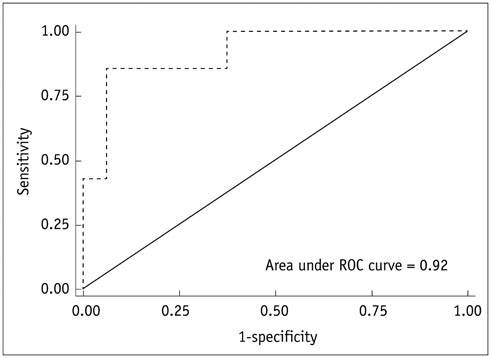
Fig. 1 Receiver operating characteristics (ROCs) curve for maximum standardized uptake value (SUVmax) for prediction of tumor grade of pulmonary mucoepidermoid carcinoma. Optimal cut-off value of SUVmax from PET/CT was calculated as 6.5 by ROCs curve. Area under curve for SUVmax was 0.92 and sensitivity and specificity for predicting tumor grade were 85.7% and 93.8%, respectively. PET/CT = positron emission tomography/computed tomography
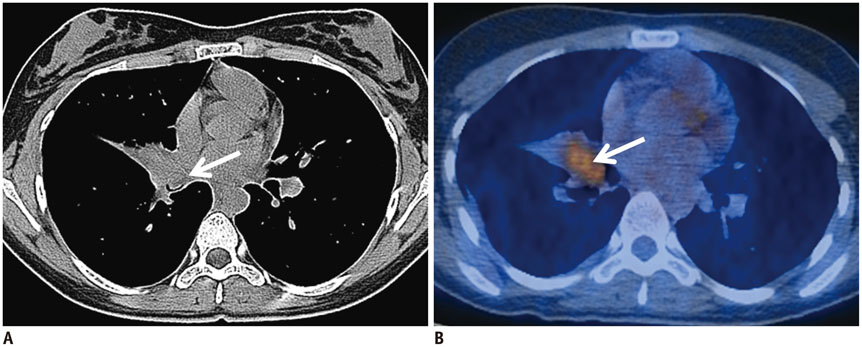
Fig. 2 Chest CT and PET/CT results for 17-year-old female with PMEC in low SUV group. A. In CT image, 14 mm intraluminal nodule (arrow) obliterated lumen of right middle lobar bronchus and protruded into lumen of intermediate bronchus. B. SUVmax of tumor in PET/CT was 4.2 (arrow) and pathologic result verified stage IA low grade PMEC. CT = computed tomography, PET/CT = positron emission tomography/computed tomography, PMEC = pulmonary mucoepidermoid carcinoma, SUV = standardized uptake value, SUVmax = maximum SUV
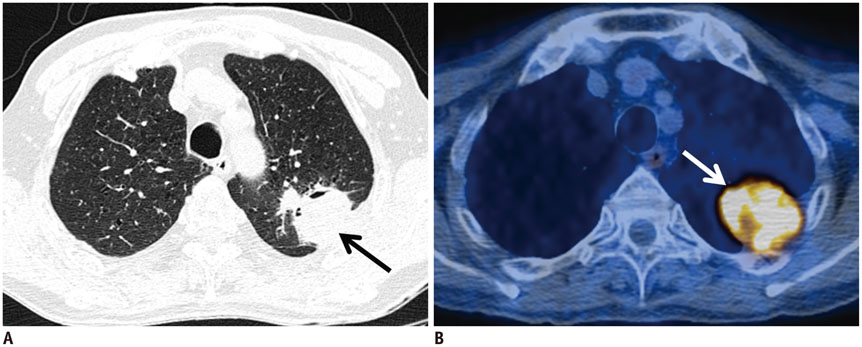
Fig. 3 Chest CT and PET/CT results for 67-year-old male with PMEC in high SUV group. A. In CT image, 53 mm mass (arrow) in left upper lobe with possibility of chest wall invasion was visible. B. SUVmax of tumor in PET/CT was 11.9 (arrow) and pathologic result verified stage IIB high grade PMEC. CT = computed tomography, PET/CT = positron emission tomography/computed tomography, PMEC = pulmonary mucoepidermoid carcinoma, SUV = standardized uptake value, SUVmax = maximum SUV
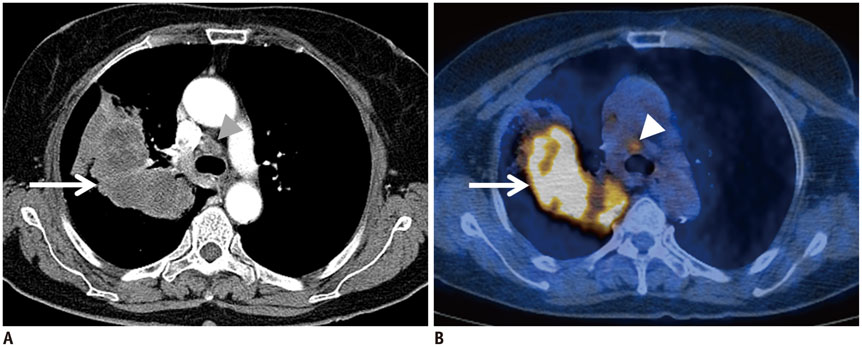
Fig. 4 Nodal metastasis of PMEC on chest CT and PET/CT in 68-year-old female. A. In CT image, 10 cm large mass (arrow) was evident in right upper lobe and mediastinal lymph nodes in para-tracheal area (arrowhead) were enlarged, representing possible nodal metastases. B. In PET/CT, SUVmax of mass was 13.1 (arrow) and slightly increased uptake in right para-tracheal lymph nodes (SUVmax = 2.9, arrowhead) were seen. Pathologic results revealed high grade PMEC with single metastasis in right lower para-tracheal lymph node representing stage IIIA. CT = computed tomography, PET/CT = positron emission tomography/computed tomography, PMEC = pulmonary mucoepidermoid carcinoma, SUVmax = maximum standardized uptake value
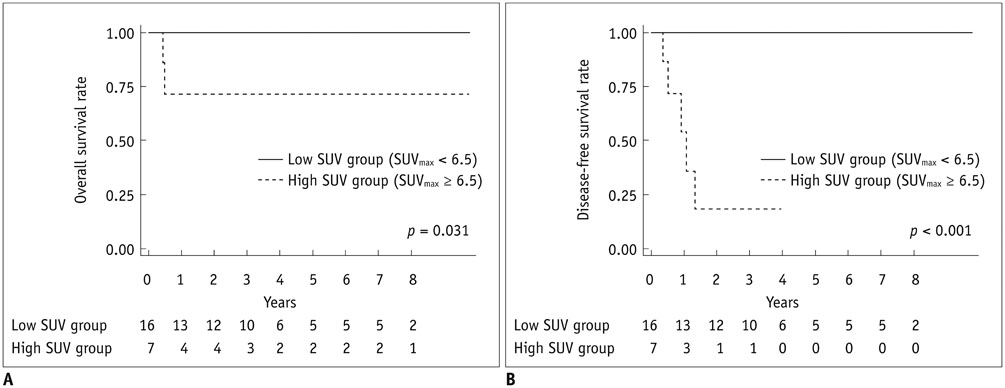
Fig. 5 Kaplan-Meier overall and disease-free survival of 23 patients after complete resection for PMEC according to SUV group. Overall survival (A) was significantly higher in low SUV group than high SUV group (5-year survival rates of 100% vs. 71.4%, p = 0.031). Disease-free survival (B) was also significantly higher in low SUV group (3-year survival rates of 100% vs. 17.9%, p < 0.001). PMEC = pulmonary mucoepidermoid carcinoma, SUV = standardized uptake value
Reference
-
1. Turnbull AD, Huvos AG, Goodner JT, Foote FW Jr. Mucoepidermoid tumors of bronchial glands. Cancer. 1971; 28:539–544.2. Leonardi HK, Jung-Legg Y, Legg MA, Neptune WB. Tracheobronchial mucoepidermoid carcinoma. Clinicopathological features and results of treatment. J Thorac Cardiovasc Surg. 1978; 76:431–443.3. Heitmiller RF, Mathisen DJ, Ferry JA, Mark EJ, Grillo HC. Mucoepidermoid lung tumors. Ann Thorac Surg. 1989; 47:394–399.4. Beasley MB, Brambilla E, Travis WD. The 2004 World Health Organization classification of lung tumors. Semin Roentgenol. 2005; 40:90–97.5. Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987; 60:1346–1352.6. Klacsmann PG, Olson JL, Eggleston JC. Mucoepidermoid carcinoma of the bronchus: an electron microscopic study of the low grade and the high grade variants. Cancer. 1979; 43:1720–1733.7. Chin CH, Huang CC, Lin MC, Chao TY, Liu SF. Prognostic factors of tracheobronchial mucoepidermoid carcinoma--15 years experience. Respirology. 2008; 13:275–280.8. Xi JJ, Jiang W, Lu SH, Zhang CY, Fan H, Wang Q. Primary pulmonary mucoepidermoid carcinoma: an analysis of 21 cases. World J Surg Oncol. 2012; 10:232.9. Zhu F, Wang W, Hou Y, Shi J, Liu Z, He D, et al. MAML2 rearrangement in primary pulmonary mucoepidermoid carcinoma and the correlation with FLT1 expression. PLoS One. 2014; 9:e94399.10. Vadasz P, Egervary M. Mucoepidermoid bronchial tumors: a review of 34 operated cases. Eur J Cardiothorac Surg. 2000; 17:566–569.11. Song Z, Liu Z, Wang J, Zhu H, Zhang Y. Primary tracheobronchial mucoepidermoid carcinoma--a retrospective study of 32 patients. World J Surg Oncol. 2013; 11:62.12. Kang DY, Yoon YS, Kim HK, Choi YS, Kim K, Shim YM, et al. Primary salivary gland-type lung cancer: surgical outcomes. Lung Cancer. 2011; 72:250–254.13. Molina JR, Aubry MC, Lewis JE, Wampfler JA, Williams BA, Midthun DE, et al. Primary salivary gland-type lung cancer: spectrum of clinical presentation, histopathologic and prognostic factors. Cancer. 2007; 110:2253–2259.14. Lee GD, Kang do K, Kim HR, Jang SJ, Kim YH, Kim DK, et al. Surgical outcomes of pulmonary mucoepidermoid carcinoma: a review of 23 cases. Thorac Cardiovasc Surg. 2014; 62:140–146.15. Brandwein MS, Ivanov K, Wallace DI, Hille JJ, Wang B, Fahmy A, et al. Mucoepidermoid carcinoma: a clinicopathologic study of 80 patients with special reference to histological grading. Am J Surg Pathol. 2001; 25:835–845.16. Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer. 1998; 82:1217–1224.17. Kinoshita H, Shimotake T, Furukawa T, Deguchi E, Iwai N. Mucoepidermal carcinoma of the lung detected by positron emission tomography in a 5-year-old girl. J Pediatr Surg. 2005; 40:E1–E3.18. Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007; 21:299–302.19. Lee EY, Vargas SO, Sawicki GS, Boyer D, Grant FD, Voss SD. Mucoepidermoid carcinoma of bronchus in a pediatric patient: (18)F-FDG PET findings. Pediatr Radiol. 2007; 37:1278–1282.20. Kuzucuoglu M, Karamustafaoglu YA, Cicin I, Yoruk Y. A rarely seen mucoepidermoid carcinoma of the left main bronchus. J Cancer Res Ther. 2014; 10:384–386.21. Jeong SY, Lee KS, Han J, Kim BT, Kim TS, Shim YM, et al. Integrated PET/CT of salivary gland type carcinoma of the lung in 12 patients. AJR Am J Roentgenol. 2007; 189:1407–1413.22. Elnayal A, Moran CA, Fox PS, Mawlawi O, Swisher SG, Marom EM. Primary salivary gland-type lung cancer: imaging and clinical predictors of outcome. AJR Am J Roentgenol. 2013; 201:W57–W63.23. Yang CS, Kuo KT, Chou TY, Lin CM, Hsu WH, Huang MH, et al. Mucoepidermoid tumors of the lung: analysis of 11 cases. J Chin Med Assoc. 2004; 67:565–570.24. Santambrogio L, Cioffi U, De Simone M, Rosso L, Ferrero S, Giunta A. Video-assisted sleeve lobectomy for mucoepidermoid carcinoma of the left lower lobar bronchus: a case report. Chest. 2002; 121:635–636.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
- Metastases to Skeletal Muscles from Non-Small Cell Lung Cancer Demonstrated by 18F-FDG PET/CT
- Esophageal Leiomyoma with intense FDG uptake on 18F-FDG PET/CT
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Lung Adenocarcinoma Staged as an Unknown Primary Presenting with Symptomatic Colon Metastases: Staging by 18F-FDG PET/CT
