Magnetic Resonance Imaging Assessment of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia in Children
- Affiliations
-
- 1Department of Diagnostic Imaging, The Hospital for Sick Children and Research Institute, University of Toronto, Ontario, Canada. shi-joon.yoo@sickkids.ca
- 2The Labatt Heart Centre, The Hospital for Sick Children and Research Institute, University of Toronto, Ontario, Canada.
- KMID: 2145526
- DOI: http://doi.org/10.4070/kcj.2010.40.8.357
Abstract
- Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) is a genetically determined disease that progresses continuously from conception and throughout life. ARVC/D manifests predominantly in young adulthood. Early identification of the concealed cases in childhood is of utmost importance for the prevention of sudden cardiac death later in life. Magnetic resonance imaging (MRI) is routinely requested in patients with a confirmed or suspected diagnosis of ARVC/D and in family members of the patients with ARVC/D. Although the utility of MRI in the assessment of ARVC/D is well recognized in adults, MRI is a low-yield test in children as the anatomical, histological, and functional changes are frequently subtle or not present in the early phase of the disease. MRI findings of ARVC/D include morphologic changes such as right ventricular dilatation, wall thinning, and aneurismal outpouchings, as well as abnormal tissue characteristics such as myocardial fibrosis and fatty infiltration, and functional abnormalities such as global ventricular dysfunction and regional wall motion abnormalities. Among these findings, regional wall motion abnormalities are the most reliable MRI findings both in children and adults, while myocardial fibrosis and fat infiltration are rarely seen in children. Therefore, an MRI protocol should be tailored according to the patient's age and compliance, as well as the presence of other findings, instead of using the protocol that is used for adults. We propose that MRI in children with ARVC/D should focus on the detection of regional wall motion abnormalities and global ventricular function by using a cine imaging sequence and that the sequences for myocardial fat and late gadolinium enhancement of the myocardium are reserved for those who show abnormal findings at cine imaging. Importantly, MRI should be performed and interpreted by experienced examiners to reduce the number of false positive and false negative readings.
Keyword
MeSH Terms
Figure
-
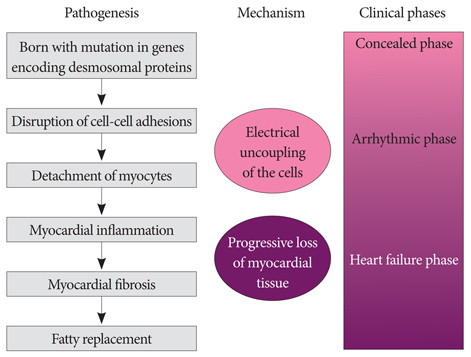
Fig. 1 Proposed pathogenesis and natural history of arrhythmogenic right ventricular cardiomyopathy/dysplasia.
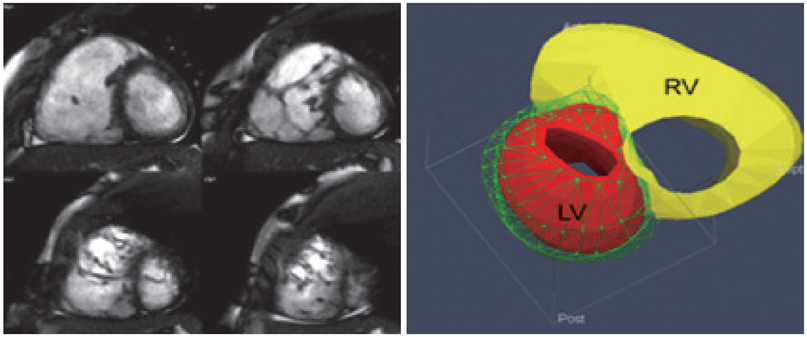
Fig. 2 Short axis cine MRI images show right ventricular dilatation and randomly oriented prominent trabeculae in the apical part of the right ventricle. The 3-dimensional volume model on the right shows significant discrepancy in right (RV) and left (LV) ventricular volumes.

Fig. 3 An axial cine image shows thinning and crinkling of the inferior part of the free wall of the RV. Small outpouchings (arrows) give rise to an appearance of an accordion. RV: right ventricle, LV: left ventricle.
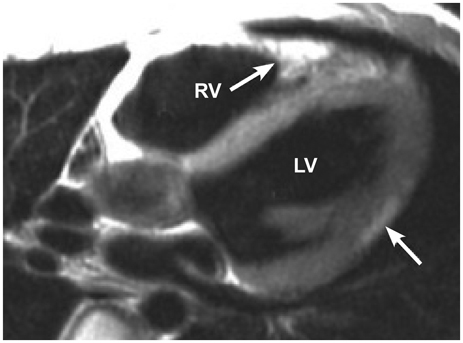
Fig. 4 A T1-weighted spin-echo image in axial plane shows a high signal intensity area in the subepicardial region of the posterior wall (arrow) of the left ventricle (LV). High signal intensity (arrow) is also seen in the moderator band of the right ventricle (RV). Both are considered fatty infiltration in the myocardium and the myocardial biopsy demonstrated fatty replacement of the myocardium.
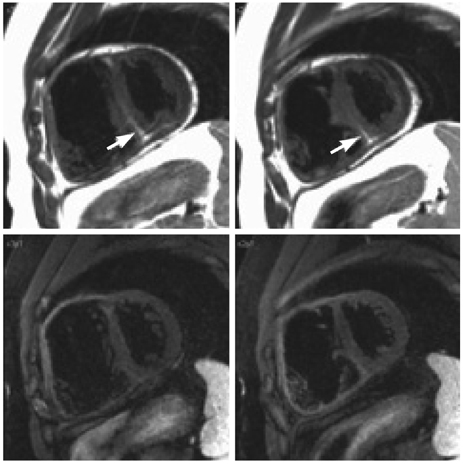
Fig. 5 Idiopathic fatty myocardium. Black blood images obtained with the double-inversion recovery technique (upper panels) show high-signal intensity fat (arrow) in the lower part of the interventricular septum. Images obtained with the triple-inversion recovery technique (lower panels) show suppression of the high intensity signals of the subcutaneous and epicardial fat as well as the myocardial fat. The patient had pulmonary atresia with intact ventricular septum and underwent surgical pulmonary valvotomy. The ventricular function was normal.

Fig. 6 A late gadolinium enhancement image shows a thinned right ventricular (RV) wall. The apical part of the thinned free wall of RV shows enhancement (arrows). A small area of enhancement (arrow) is also seen in the posterior wall of the left ventricle (LV).
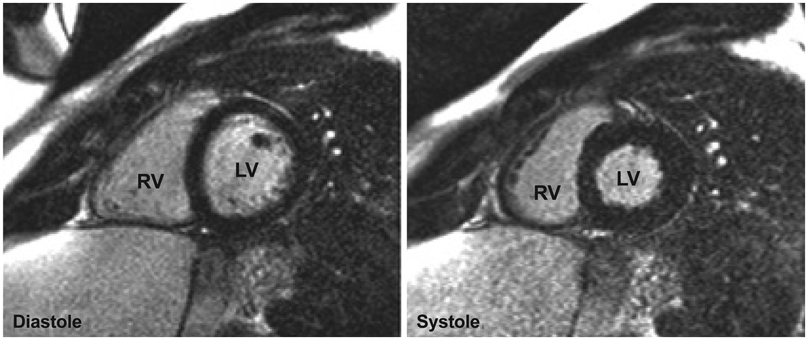
Fig. 7 Late gadolinium enhancement images obtained in diastole (left panel) and in systole (right panel) in a normal individual. Note that the myocardium of the free wall of the RV is better defined in systole than in diastole. RV: right ventricle, LV: left ventricle.
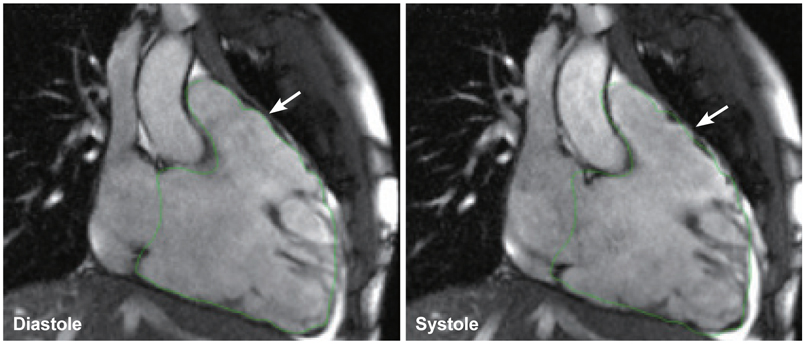
Fig. 8 Cine images in 2-chamber view of the right ventricle show right ventricular dilatation, poor systolic function, and dyskinesia of the anterior wall of the right ventricular outflow tract (arrow). The right ventricular contour was drawn on the diastolic image as shown in the left panel. The contour was copied and overlain on the systolic image as shown in the right panel. Note the minimal downward excursion of the base of the right ventricle in systole. The anterior wall of the right ventricular outflow tract shows protrusion in systole beyond the limit of right ventricular contour drawn on the diastolic image.
Cited by 1 articles
-
Comparison of CMR Findings according to the Presence or Absence of Isolated Focal Right Ventricular Dyskinetic Segments in Patients with Clinical Suspicion of ARVC
Sung Min Ko
J Cardiovasc Imaging. 2019;27(2):102-104. doi: 10.4250/jcvi.2019.27.e24.
Reference
-
1. Tabib A, Loire R, Chalabreysse L, et al. Circumstances of death and gross and microscopic observations in a series of 200 cases of sudden death associated with arrhythmogenic right ventricular cardiomyopathy and/or dysplasia. Circulation. 2003. 108:3000–3005.2. Basso C, Corrado D, Marcus RI, Nava A, Thiene G. Arrhythmogenic right ventricular cardiomyopathy. Lancet. 2009. 373:1289–1300.3. Corrado D, Basso C, Thine G. Arrhythmogenic right ventricular cardiomyopathy: an update. Heart. 2009. 95:766–773.4. Hamilton RM, Fidler L. Right ventricular cardiomyopathy in the young: an emerging challenge. Heart Rhythm. 2009. 6:571–575.5. Saffitz JE. Desmosome mutations in arrhythmogenic right ventricular cardiomyopathy: important insight but only part of the future. Circ Cardiovasc Genet. 2009. 2:415–417.6. Sen-Chowdhry S, Syrris P, McKenna WJ. Role of genetic analysis in the management of patients with arrhythmogenic right ventricular dysplasia/ cardiomyopathy. J Am Coll Cardiol. 2007. 50:1813–1821.7. Bhuiyan ZA, Jonboed JD, van der Smagt J, et al. Desmoglein-2 and desmocollin-2 mutations in Dutch arrhythmogenic right ventricular dysplasia/ cardiomyopathy patients: result from a multicenter study. Circ Cardiovasc Genet. 2009. 2:418–427.8. den Haan AD, Tan BY, Zikusoka MN, et al. Comprehensive desmosome mutation analysis in north Americans with arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circ Cardiovasc Genet. 2009. 2:428–435.9. Hershberger RE, Cowan J, Morales A, Sigfried JD. Screening, counseling, and testing in dilated, hypertrophic, and arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circ Heart Fail. 2009. 2:253–261.10. Sen-Chowdhry S, Syrris P, Ward D, Asimaki A, Sevdalis E, McKenna WJ. Clinical and genetic characterization of families with arrhythmogenic right ventricular dysplasia/cardiomyopathy provides novel insights into patterns of disease expression. Circulation. 2007. 115:1710–1720.11. Turrini P, Corrado D, Basso C, Nava A, Thiene G. Noninvasive risk stratification in arrhythmogenic right ventricular cardiomyopathy. Ann Noninvasive Electrocardiol. 2003. 8:161–169.12. Hulot JS, Jouven X, Empana JP, Frank R, Fontaine G. Natural history and risk stratification of arrhythmogenic right ventricular dysplasia/ cardiomyopathy. Circulation. 2004. 110:1879–1884.13. Sen-Chowdhry S, Morgan RD, Chambers JC, McKenna WJ. Arrhythmogenic cardiomyopathy: etiology, diagnosis, and treatment. Annu Rev Med. 2010. 61:233–253.14. Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA. 2006. 296:1593–1601.15. Thiene G, Carturan E, Corrado D, Basso C. Prevention of sudden cardiac death in the young and in athletes: dream or reality? Cardiovasc Pathol. 2009. [Epub ahead of print].16. Corrado D, Pelliccia A, Heidbuchel H, et al. Recommendations for interpretation of 12-lead electrocardiogram in the athlete. Eur Heart J. 2010. 31:243–259.17. Marcus FI, Zareba W, Calkins H, et al. Arrhythmogenic right ventricular cardiomyopathy/dysplasia clinical presentation and diagnostic evaluation: results from the North American Multidisciplinary Study. Heart Rhythm. 2009. 6:984–992.18. McKenna WJ, Thiene G, Nava A, et al. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Br Heart J. 1994. 71:215–218.19. Marcus FI, McKenna WJ, Sherrill D, et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the Task Force Criteria. Circulation. 2010. 121:1533–1541. Eur Heart J 2010;31:806-14.20. Asimaki A, Tandri H, Huang H, et al. A new diagnostic test for arrhythmogenic right ventricular cardiomyopathy. N Engl J Med. 2009. 360:1075–1084.21. Tandri H, Macedo R, Calkins H, et al. Role of magnetic resonance imaging in arrhythmogenic right ventricular dysplasia: insights from the North American arrhythmogenic right ventricular dysplasia (ARVD/C) study. Am Heart J. 2008. 155:147–153.22. Tandri H, Saranathan M, Rodriguez ER, et al. Noninvasive detection of myocardial fibrosis in arrhythmogenic right ventricular cardiomyopathy using delayed-enhancement magnetic resonance imaging. J Am Coll Cardiol. 2005. 45:98–103.23. Dalal D, Tandri H, Judge DP, et al. Morphologic variants of familial arrhythmogenic right ventricular dysplasia/cardiomyopathy: a genetics-magnetic resonance imaging correlation study. J Am Coll Cardiol. 2009. 53:1289–1299.24. Tandri H, Calkins H, Nasir K, et al. Magnetic resonance imaging findings in patients meeting task force criteria for arrhythmogenic right ventricular dysplasia. J Cardiovasc Electrophysiol. 2003. 14:476–482.25. Groenink M, Wilde AA. The "accordion sign" a new tune in arrhythmogenic right ventricular dysplasia/cardiomyopathy magnetic resonance imaging? J Am Coll Cardiol. 2009. 53:1300–1301.26. Ricci C, Longo R, Pagnan L, et al. Magnetic resonance imaging in right ventricular dysplasia. Am J Cardiol. 1992. 70:1589–1595.27. Auffermann W, Wichter T, Breithardt G, Joachimsen K, Peters PE. Arrhythmogenic right ventricular disease: MR imaging vs. angiography. AJR Am J Roentgenol. 1993. 161:549–555.28. Blake LM, Scheinman MM, Higgins CB. MR features of arrhythmognic right ventricular dysplasia. AJR Am J Roentgenol. 1994. 162:809–812.29. Molinari G, Sardanelli F, Gaita F, et al. Right ventricular dysplasia as a generalized cardiomyopathy?: findings on magnetic resonance imaging. Eur Heart J. 1995. 16:1619–1624.30. Kayser HW, van der Wall EE, Sivananthan MU, Plein S, Bloomer TN, de Roos A. Diagnosis of arrhythmogenic right ventricular dysplasia: a review. Radiographics. 2002. 22:639–648.31. Castillo E, Tandri H, Rodriguez ER, et al. Arrhythmogenic right ventricular dysplasia: ex vivo and in vivo fat detection with black-blood MR imaging. Radiology. 2004. 232:38–48.32. Bluemke DA, Krupinski EA, Ovitt T, et al. MR imaging of arrhythmogenic right ventricular cardiomyopathy: morphologic findings and interobserver reliability. Cardiology. 2003. 99:153–162.33. Tandri H, Castillo E, Ferrari VA, et al. Magnetic resonance imaging of arrhythmogenic right ventricular dysplasia: sensitivity, specificity, and observer variability of fat detection versus functional analysis of the right ventricle. J Am Coll Cardiol. 2006. 48:2277–2284.34. Burke AP, Farb A, Tashko G, Virmani R. Arrhythmogenic right ventricular cardiomyopathy and fatty replacement of the right ventricular myocardium: are they different diseases? Circulation. 1998. 97:1571–1580.35. Fontaine G, Fontaliran F, Zenati O, et al. Fat in the heart: a feature unique to the human species? Observational reflections on an unsolved problem. Acta Cardiol. 1999. 54:189–194.36. Macedo R, Prakasa K, Tichnell C, et al. Marked lipomatous infiltration of the right ventricle: MRI findings in relation to arrhythmogenic right ventricular dysplasia. AJR Am J Roentgenol. 2007. 188:W423–W427.37. Hunold P, Wieneke H, Bruder O, et al. Late enhancement: a new feature in MRI of arrhythmogenic right ventricular cardiomyopathy? J Cardiovasc Magn Reson. 2005. 7:649–655.38. Sen-Chowdhry S, Prasad SK, Syrris P, et al. Cardiovascular magnetic resonance in arrhythmogenic right ventricular cardiomyopathy revisited: comparison with task force criteria and genotype. J Am Coll Cardiol. 2006. 48:2132–2140.39. Grosse-Wortmann L, Macgowan CK, Vidarsson L, Yoo SJ. Late gadolinium enhancement of the right ventricular myocardium: is it really different from the left? J Cardiovasc Magn Reson. 2008. 10:20.40. Hamdan A, Thouet T, Sebastian K, et al. Regional right ventricular function and timing of contraction in healthy volunteers evaluated by strain-encoded MRI. J Magn Reson Imaging. 2008. 28:1379–1385.41. Jain A, Shehata ML, Stuber M, et al. Prevalence of left ventricular regional dysfunction in arrhythmogenic right ventricular dysplasia: a tagged MRI study. Circ Cardiovasc Imaging. 2010. 3:290–297.42. Sen-Chowdhry S, McKenna WJ. The utility of magnetic resonance imaging in the evaluation of arrhtymogenic right ventricular cardiomyopathy. Curr Opin Cardiol. 2008. 23:38–45.43. Fogel MA, Weinberg PM, Harris M, Rhodes L. Usefulness of magnetic resonance imaging for the diagnosis of right ventricular dysplasia in children. Am J Cardiol. 2006. 97:1232–1237.44. Aviram G, Fishman JE, Young ML, Redha E, Biliciler-Denktas G, Rodriguez MM. MR evaluation of arrhythmogenic right ventricular cardiomyopathy in pediatric patients. AJR Am J Roentgenol. 2003. 180:1135–1141.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of arrhythmogenic right ventricular cardiomyopathy/dysplasia involving the left ventricle
- A Case of Arrhythmogenic Right Ventricular Dysplasia
- Catheter Ablation of Ventricular Tachycardia/Fibrillation in a Patient with Right Ventricular Amyloidosis with Initial Manifestations Mimicking Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy
- A Case of Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy with Cardiac Arrest in the Emergency Department
- Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy: Report of an Autopsy Case
