Aortic Aneurysm Screening in a High-Risk Population: A Non-Contrast Computed Tomography Study in Korean Males with Hypertension
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Seoul, Korea. hjchang@yuhs.ac
- 2Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2145477
- DOI: http://doi.org/10.4070/kcj.2014.44.3.162
Abstract
- BACKGROUND AND OBJECTIVES
Screening strategies for aortic aneurysm (AA) according to risk factors and ethnicity are controversial. This study explored the prevalence of AA and determined whether screening is necessary in a population of multiple risk factors.
SUBJECTS AND METHODS
From June, 2012 to April, 2013, 542 consecutive elderly (> or =65 years) male hypertensive patients without a history of AA were prospectively enrolled. After excluding 15 patients (2.8%) with aortic valve surgery, 30 patients (5.5%) with suboptimal computed tomography (CT) images, the remaining 496 patients (age 73+/-5 years) comprised the study population. Maximal diameters of the thoracic and abdominal aorta were measured using non-contrast CT.
RESULTS
The prevalence of thoracic AA (TAA, diameter > or =40 mm) and abdominal AA (AAA, diameter > or =30 mm) was 36.5% (181/496) and 6.0% (30/496), respectively. In the multivariate logistic regression analysis, determinants for TAA were age {odds ratio (OR) 1.059, 95% confidence interval (CI) 1.018-1.101, p=0.005}, dyslipidemia (OR 0.621, 95% CI 0.418-0.923, p=0.018), body surface area (OR 11.92, 95% CI 2.787-50.97, p=0.001), diastolic blood pressure (OR 1.029, 95% CI 1.009-1.049, p=0.004) and AAA (OR 3.070, 95% CI 1.398-6.754, p=0.005). In contrast, AAA was independently associated with dysplipidemia (OR 2.792, 95% CI 1.091-7.143, p=0.032), current/past smokerfs (OR 4.074, 95% CI 1.160-14.31, p=0.028), and TAA (OR 3.367, 95% CI 1.550-7.313, p=0.002).
CONCLUSION
The prevalence of AA was significant and TAA was more prevalent than AAA in elderly Korean males with hypertension. Future research should establish distinct screening strategies for TAA and AAA according to risk factors and ethnicity.
Keyword
MeSH Terms
Figure
-
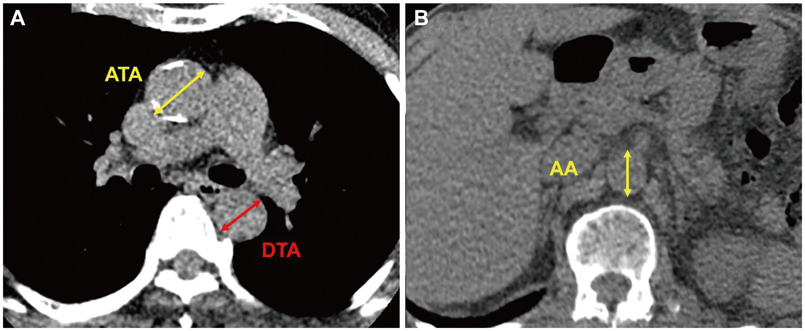
Fig. 1 Measurement of aortic diameter in the axial plane. Ascending and descending thoracic aorta (A) and abdominal aorta (B). ATA: ascending thoracic aorta, DTA: descending thoracic aorta, AA: abdominal aorta.
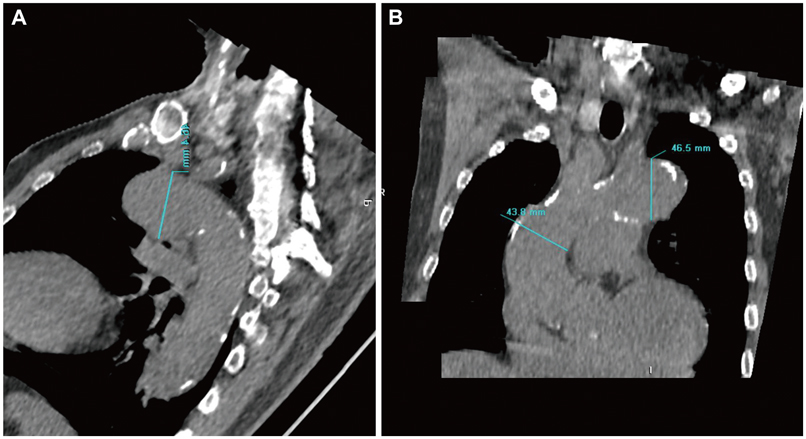
Fig. 2 Reconstructed images of aorta using non-contrast computed tomography. Reconstructed sagittal (A) and coronal (B) images of aorta.

Fig. 3 Histogram of maximal thoracic (A) and abdominal aorta (B). Red lines indicate maximal thoracic aorta of 40 mm and maximal abdominal aorta of 30 mm. TAMAX: maximal thoracic aorta, AAMAX: maximal abdominal aorta.

Fig. 4 Prevalence of thoracic aortic aneurysm in patients with and without abdominal aortic aneurysm. TAA (-), patients without thoracic aortic aneurysm; TAA (+), patients with thoracic aortic aneurysm; AAA (+), patients with abdominal aortic aneurysm; AAA (-), patients without abdominal aortic aneurysm.

Fig. 5 Prevalence of thoracic aortic aneurysm (A) and abdominal aortic aneurysm (B) according to history of smoking. Smoking (+), current or past smoker; Smoking (-), never smoked.
Reference
-
1. Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J Am Coll Cardiol. 2010; 55:841–857.2. Isselbacher EM. Thoracic and abdominal aortic aneurysms. Circulation. 2005; 111:816–828.3. Lindholt JS, Henneberg EW, Fasting H, Juul S. Mass or high-risk screening for abdominal aortic aneurysm. Br J Surg. 1997; 84:40–42.4. Clouse WD, Hallett JW Jr, Schaff HV, et al. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc. 2004; 79:176–180.5. Acosta S, Ogren M, Bengtsson H, Bergqvist D, Lindblad B, Zdanowski Z. Increasing incidence of ruptured abdominal aortic aneurysm: a population-based study. J Vasc Surg. 2006; 44:237–243.6. Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol. 2010; 56:1864–1894.7. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; Trans-Atlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006; 113:e463–e654.8. Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg. 2002; 74:S1877–S1880. discussion S1892-8.9. Davies RR, Goldstein LJ, Coady MA, et al. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg. 2002; 73:17–27. discussion 27-8.10. Wolak A, Gransar H, Thomson LE, et al. Aortic size assessment by noncontrast cardiac computed tomography: normal limits by age, gender, and body surface area. JACC Cardiovasc Imaging. 2008; 1:200–209.11. Mao SS, Ahmadi N, Shah B, et al. Normal thoracic aorta diameter on cardiac computed tomography in healthy asymptomatic adults: impact of age and gender. Acad Radiol. 2008; 15:827–834.12. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter Cardiovasc Interv. 2010; 76:E43–E86.13. Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006; 114:2611–2618.14. Rizzo JA, Coady MA, Elefteriades JA. Procedures for estimating growth rates in thoracic aortic aneurysms. J Clin Epidemiol. 1998; 51:747–754.15. Jamrozik K, Norman PE, Spencer CA, et al. Screening for abdominal aortic aneurysm: lessons from a population-based study. Med J Aust. 2000; 173:345–350.16. Singh K, Bønaa KH, Jacobsen BK, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The Tromsø Study. Am J Epidemiol. 2001; 154:236–244.17. Takei H, Ishikawa S, Otaki A, et al. Screening for abdominal aortic aneurysm and occlusive peripheral vascular disease in Japanese residents. Surg Today. 1995; 25:608–611.18. Adachi K, Iwasawa T, Ono T. Screening for abdominal aortic aneurysms during a basic medical checkup in residents of a Japanese rural community. Surg Today. 2000; 30:594–599.19. Poon JT, Cheng SW, Wong JS, Ting AC. Prevalence of abdominal aortic aneurysm in Chinese patients with severe coronary artery disease. ANZ J Surg. 2010; 80:630–633.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Study of Surgical Treatment of Aortic Aneurysm
- Acute Aortic Syndrome: Recent Trends in Imaging Assessment Using Computed Tomography Angiography
- Role of PET/CT in the Evaluation of Aortic Disease
- Use of Percutaneous Endovascular Stent Graft in Patients with Thoracic Aortic Aneurysm
- Stented Aortic Graft Insertion in an Infrarenal Abdominal Aortic Aneurysm as Performed by Cardiovascular Surgeons: Report of 3 cases
