Stress-Induced Cardiomyopathy: The Role of Echocardiography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Wonju College of Medicine, Yonsei University, Wonju, Korea. kimjy@yonsei.ac.kr
- KMID: 2135425
- DOI: http://doi.org/10.4250/jcu.2011.19.1.7
Abstract
- Echocardiography is widely used to carry out non-invasive cardiac evaluation at the bedside and provides useful real-time information about hemodynamics. It can also be used to diagnose a stress-induced cardiomyopathy and its complications such as shock, heart failure and apical thrombus. Early diagnosis and management are important to prevent possible complications, and short-term follow-up by echocardiography can readily determine the improvement in these abnormalities. In this brief review, we summarize the role of echocardiography in stress-induced cardiomyopathy, with a special focus on its benefits in the era of new emerging diagnostic technology.
MeSH Terms
Figure
-

Fig. 1 Apical four chamber view shows ballooning on LV apex with RV involvement and biatrial enlargement (A). On color Doppler, moderate TR is detected (B) and peak TR velocity is 3.3 m/s with a derived systolic pulmonary arterial systolic pressure of 44 mmHg (C). LV: left ventricle, RV: right ventricle, TR: tricuspid regurgitation.
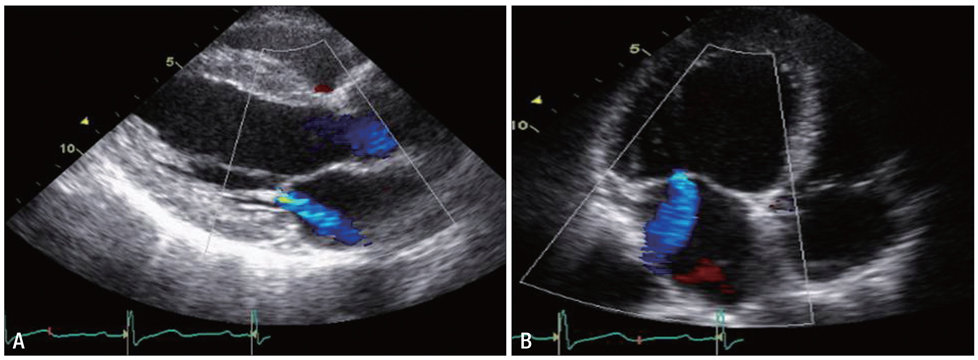
Fig. 2 Moderate mitral regurgitation detected by parasternal long axis view (A) and apical four chamber view (B).

Fig. 3 Mid-ventricular ballooning with preserved basal and apical contractility is observed using echocardiography (A and B) and left ventriculography (C and D).
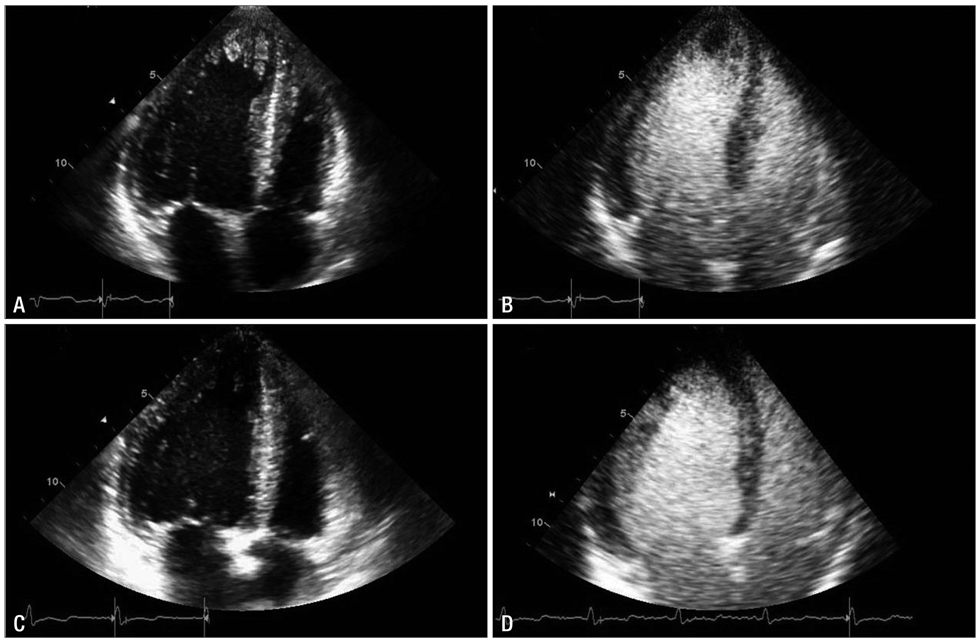
Fig. 4 Echocardiography shows a left ventricular (LV) apical thrombus on an apical four-chamber view (A) and contrast echocardiography confirms a filling defect of the LV thrombus (B). Follow-up echocardiography (C and D) shows no residual thrombus.
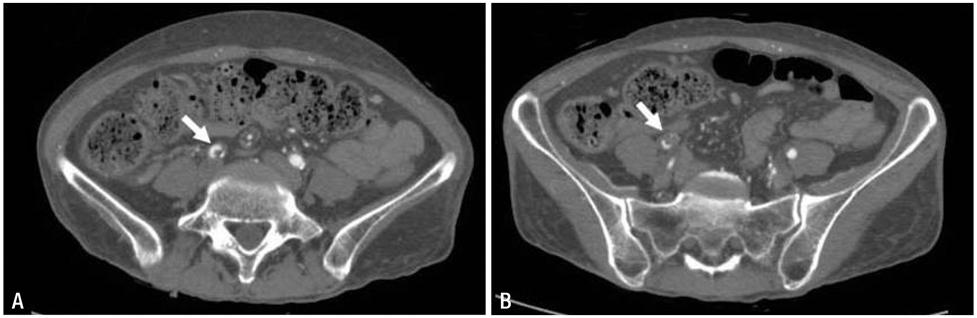
Fig. 5 Multiple thrombi (arrow) are detected in the right common iliac artery (A) and right external iliac artery (B) on abdominal CT.
Cited by 1 articles
-
Diagnosis and Management of Stress-induced Cardiomyopathy in Neurological Intensive Care Units
So-Ryoung Lee, Yeonyee E. Yoon
J Neurocrit Care. 2015;8(1):1-8. doi: 10.18700/jnc.2015.8.1.1.
Reference
-
1. Grawe H, Katoh M, Kuhl HP. Stress cardiomyopathy mimicking acute coronary syndrome: case presentation and review of the literature. Clin Res Cardiol. 2006. 95:179–185.
Article2. Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, Yoshiyama M, Miyazaki S, Haze K, Ogawa H, Honda T, Hase M, Kai R, Morii I. Angina Pectoris-Myocardial Infarction Investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina pectoris-myocardial infarction investigations in Japan. J Am Coll Cardiol. 2001. 38:11–18.
Article3. Nef HM, Mollmann H, Akashi YJ, Hamm CW. Mechanisms of stress (Takotsubo) cardiomyopathy. Nat Rev Cardiol. 2010. 7:187–193.
Article4. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006. 27:1523–1529.
Article5. Pernicova I, Garg S, Bourantas CV, Alamgir F, Hoye A. Takotsubo cardiomyopathy: a review of the literature. Angiology. 2010. 61:166–173.
Article6. Bybee KA, Prasad A, Barsness GW, Lerman A, Jaffe AS, Murphy JG, Wright RS, Rihal CS. Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am J Cardiol. 2004. 94:343–346.
Article7. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008. 155:408–417.
Article8. Hurst RT, Askew JW, Reuss CS, Lee RW, Sweeney JP, Fortuin FD, Oh JK, Tajik AJ. Transient midventricular ballooning syndrome: a new variant. J Am Coll Cardiol. 2006. 48:579–583.9. Van de Walle SO, Gevaert SA, Gheeraert PJ, De Pauw M, Gillebert TC. Transient stress-induced cardiomyopathy with an "inverted takotsubo" contractile pattern. Mayo Clin Proc. 2006. 81:1499–1502.
Article10. Elesber AA, Prasad A, Bybee KA, Valeti U, Motiei A, Lerman A, Chandrasekaran K, Rihal CS. Transient cardiac apical ballooning syndrome: prevalence and clinical implications of right ventricular involvement. J Am Coll Cardiol. 2006. 47:1082–1083.
Article11. Haghi D, Athanasiadis A, Papavassiliu T, Suselbeck T, Fluechter S, Mahrholdt H, Borggrefe M, Sechtem U. Right ventricular involvement in Takotsubo cardiomyopathy. Eur Heart J. 2006. 27:2433–2439.
Article12. Winchester DE, Ragosta M, Taylor AM. Concurrence of angiographic coronary artery disease in patients with apical ballooning syndrome (tako-tsubo cardiomyopathy). Catheter Cardiovasc Interv. 2008. 72:612–616.
Article13. Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010. 55:333–341.
Article14. Lee PH, Song JK, Sun BJ, Choi HO, Seo JS, Na JO, Kim DH, Song JM, Kang DH, Kim JJ, Park SW. Outcomes of patients with stress-induced cardiomyopathy diagnosed by echocardiography in a tertiary referral hospital. J Am Soc Echocardiogr. 2010. 23:766–771.
Article15. El Mahmoud R, Mansencal N, Pilliere R, Leyer F, Abbou N, Michaud P, Nallet O, Digne F, Lacombe P, Cattan S, Dubourg O. Prevalence and characteristics of left ventricular outflow tract obstruction in Tako-Tsubo syndrome. Am Heart J. 2008. 156:543–548.
Article16. Merli E, Sutcliffe S, Gori M, Sutherland GG. Tako-Tsubo cardiomyopathy: new insights into the possible underlying pathophysiology. Eur J Echocardiogr. 2006. 7:53–61.
Article17. Parodi G, Del Pace S, Salvadori C, Carrabba N, Olivotto I, Gensini GF. Left ventricular apical ballooning syndrome as a novel cause of acute mitral regurgitation. J Am Coll Cardiol. 2007. 50:647–649.
Article18. Haghi D, Rohm S, Suselbeck T, Borggrefe M, Papavassiliu T. Incidence and clinical significance of mitral regurgitation in Takotsubo cardiomyopathy. Clin Res Cardiol. 2010. 99:93–98.
Article19. Park HE, Kim JH, Yoon YE, Park JB, Lee W, Cho Y, Heo EY, Kim HK, Kim YJ, Sohn DW. A unique case of transient midventricular ballooning: an atypical manifestation of stress-induced cardiomyopathy involvoing both ventricles. Korean Circ J. 2008. 38:677–680.
Article20. Ibanez B, Benezet-Mazuecos J, Navarro F, Farre J. Takotsubo syndrome: a Bayesian approach to interpreting its pathogenesis. Mayo Clin Proc. 2006. 81:732–735.
Article21. Akashi YJ, Tejima T, Sakurada H, Matsuda H, Suzuki K, Kawasaki K, Tsuchiya K, Hashimoto N, Musha H, Sakakibara M, Nakazawa K, Miyake F. Left ventricular rupture associated with Takotsubo cardiomyopathy. Mayo Clin Proc. 2004. 79:821–824.
Article22. Heggemann F, Weiss C, Hamm K, Kaden J, Suselbeck T, Papavassiliu T, Borggrefe M, Haghi D. Global and regional myocardial function quantification by two-dimensional strain in Takotsubo cardiomyopathy. Eur J Echocardiogr. 2009. 10:760–764.
Article23. Meimoun P, Malaquin D, Benali T, Boulanger J, Zemir H, Tribouilloy C. Transient impairment of coronary flow reserve in tako-tsubo cardiomyopathy is related to left ventricular systolic parameters. Eur J Echocardiogr. 2009. 10:265–270.
Article24. Lee JW, Kim JY, Youn YJ, Sung JK, Lee NS, Lee KH, Yoo BS, Lee SH, Yoon J, Choe KH. Clinical characteristics and prognostic factors of stress-induced cardiomyopathy. Korean Circ J. 2010. 40:277–282.
Article25. Abdelmoneim SS, Mankad SV, Bernier M, Dhoble A, Hagen ME, Ness SA, Chandrasekaran K, Pellikka PA, Oh JK, Mulvagh SL. Microvascular function in Takotsubo cardiomyopathy with contrast echocardiography: prospective evaluation and review of literature. J Am Soc Echocardiogr. 2009. 22:1249–1255.
Article26. Uznańska B, Plewka M, Wierzbowska-Drabik K, Chrzanowski Ł, Kasprzak JD. Early prediction of ventricular recovery in Takotsubo syndrome using stress and contrast echocardiography. Med Sci Monit. 2009. 15:CS89–CS94.27. Fujikawa M, Iwasaka J, Oishi C, Ueyama T, Park H, Yamamoto Y, Otani H, Iwasaka T. Three-dimensional echocardiographic assessment of left ventricular function in takotsubo cardiomyopathy. Heart Vessels. 2008. 23:214–216.
Article28. Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004. 141:858–865.
Article29. Haghi D, Papavassiliu T, Heggemann F, Kaden JJ, Borggrefe M, Suselbeck T. Incidence and clinical significance of left ventricular thrombus in tako-tsubo cardiomyopathy assessed with echocardiography. QJM. 2008. 101:381–386.
Article30. Buchholz S, Ward MR, Bhindi R, Nelson GI, Figtree GA, Grieve SM. Cardiac thrombi in stress (tako-tsubo) cardiomyopathy: more than an apical issue? Mayo Clin Proc. 2010. 85:863–864.
Article31. de Gregorio C, Grimaldi P, Lentini C. Left ventricular thrombus formation and cardioembolic complications in patients with Takotsubo-like syndrome: a systematic review. Int J Cardiol. 2008. 131:18–24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Unique Case of Transient Midventricular Ballooning: An Atypical Manifestation of Stress-Induced Cardiomyopathy Involving Both Ventricles
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
- Recurrent fetal postpartum stress induced cardiomyopathy after normal vaginal delivery
- Acute Coronary Syndrome Mimicking Atypical Stress-Induced Cardiomyopathy in a Patient with Panhypopituitarism
- Stress Related Cardiomyopathy during Flexible Bronchoscopy
