J Korean Med Assoc.
2004 Jan;47(1):85-98. 10.5124/jkma.2004.47.1.85.
Evidence-based Treatment of Peptic Ulcer Disease
- Affiliations
-
- 1Department of Internal Medicine, Division of Gastroenterology, University of Ulsan College of Medicine, Asan Medical Center, Korea. jhkm@amc.seoul.kr
- KMID: 2127830
- DOI: http://doi.org/10.5124/jkma.2004.47.1.85
Abstract
- Before the discovery of H. pylori, the therapy of peptic ulcer disease(PUD) was focused on the acid secretion. Although acid secretion is still important in the pathogenesis of PUD, eradication of H. pylori and therapy/prevention of NSAIDinduced disease is the mainstay of therapy these days. Multiple drugs have been evaluated in the therapy of H. pylori. No single agent is effective in eradicating the organism. Combination therapy for 10 to 14 days provides the greatest efficacy. The combination of two antibiotics among amoxicillin, metronidazole and clarithromycin plus either a PPI or bismuth compound(RBC: ranitidine bismuth citrate) has comparable success rates. Medical intervention for NSAIDrelated mucosal injury includes treatment of an active ulcer and prevention of future injury. Ideally the injurious agent should be stopped as the first step in the therapy of an active NSAIDinduced ulcer. If that is possible, then treatment with one of the acid inhibitory agents (H2 blockers, PPIs) is indicated. Cessation of NSAIDs is not always possible because of the patient's severe underlying disease. Only PPIs can heal GUs or DUs, independent of whether NSAIDs are discontinued. Prevention of NSAIDinduced ulceration can be accomplished by misoprostol (200 microgram qid) or a PPI. The use of COX2 specific inhibitor may also reduce injury to gastric mucosa. H. pylorinegative idiopathic peptic ulcer disease appears to be increasing. Antisecretory drugs remain the mainstay of treatment for promoting healing of idiopathic peptic ulceration. However, in the absence of H. pylori infection, antisecretory drugs are less effective in inhibiting gastric acidity. Managment of idiopathic PUD needs to be further de-fined and will require new clinical studies.
Keyword
MeSH Terms
-
Amoxicillin
Anti-Bacterial Agents
Anti-Inflammatory Agents, Non-Steroidal
Bismuth
Clarithromycin
Duodenal Ulcer
Gastric Acid
Gastric Mucosa
Helicobacter pylori
Metronidazole
Misoprostol
Peptic Ulcer*
Ranitidine
Stomach Ulcer
Ulcer
Amoxicillin
Anti-Bacterial Agents
Anti-Inflammatory Agents, Non-Steroidal
Bismuth
Clarithromycin
Metronidazole
Misoprostol
Ranitidine
Figure
-
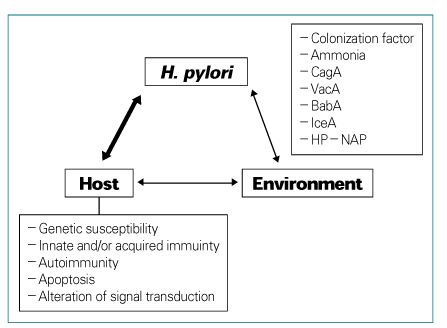
Figure 1
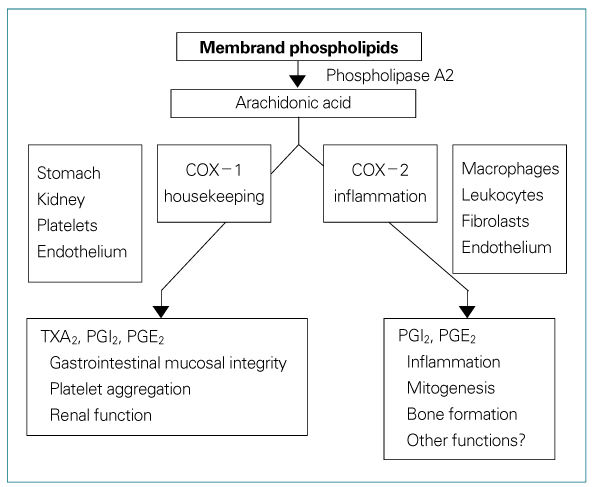
Figure 2 COX-1 and COX-2

Figure 3
Reference
-
1. Harrison's Principles of Internal Medeicine. 2001. 15th ed. 1649–1665.2. Chapter 40 : Peptic ulcer disease and its complications. Sleisenger & Fordtran's Gastrointestinal and Liver Disease. 2002. 7th ed.5. Quan C, Talley NJ. Management of peptic ulcer disease not related to Helicobacter pylori or NSAIDs. Am J Gastroenterol. 2002. 97:2950–2961.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and Treatment of Peptic Ulcer Disease: Present and Future Perspective
- The Endoscopic Diagnosis of Peptic Ulcer Disease
- Endoscopic Management of Peptic Ulcer Bleeding
- Management of Peptic Ulcer Bleeding in Patients Taking Aspirin or Anticoagulant
- A clinical review of the 188 cases of peptic ulcer perforations
