Common and Uncommon Conditions of Breast Disease in Children and Adolescents: A Pictorial Review
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Daejeon, Korea. kskim@eulji.ac.kr
- 2Department of Radiology, Dankook University Hospital, Cheonan, Korea.
- 3Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2097992
- DOI: http://doi.org/10.3348/jksr.2013.68.2.141
Abstract
- The purpose of this study is to review various breast diseases in children and adolescents and to illustrate the sonographic findings. We reviewed the cases at our institution in order to identify breast disease in children and adolescent patients who underwent sonography and mammography. Breast disease in children and adolescents included developmental disturbance, infection, benign tumors and inherent defects. In contrast to adults, the radiologic findings of malignant breast conditions in pediatric populations have rarely been reported; however, we show ductal carcinoma in situ with juvenile fibroadenoma and rhabdomyosarcoma. During childhood and adolescence, the recognition and correct identification of physiologic breast development and specific lesions in breast entities on radiologic findings is most helpful in identifying and characterizing abnormalities and in guiding further investigation.
MeSH Terms
Figure
-
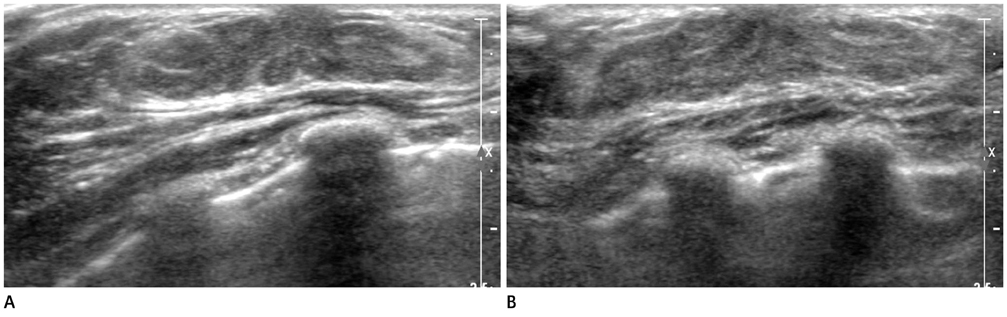
Fig. 1 Premature thelarche, 2-year-old female baby who presented with prominent both breasts. A, B. Sonogram (A, B) shows bilateral development of fibroglandular tissue at the subareolar area and there is no evidence of discrete lesion. This findings are typical premature thelarche. HAND simple radiography and pelvis sonography was normal.
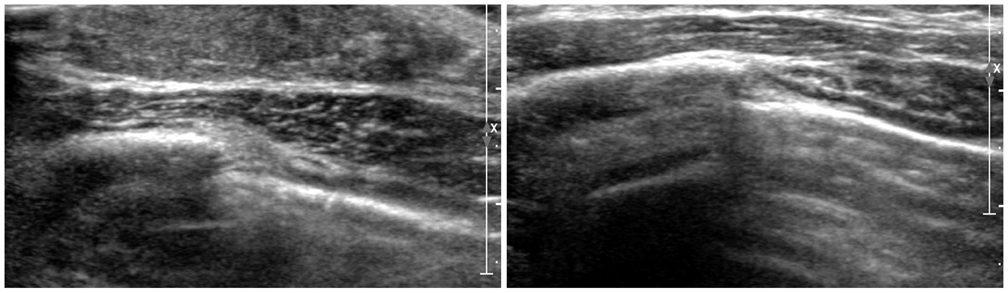
Fig. 2 Unilateral nodular gynecomastia, right breast, 17-year-old boy. A. Longitudinal sonogram shows a retroareolar discoid hypoechoic area surrounding by fatty tissue at the right breast. B. Sonogram shows normal left breast.
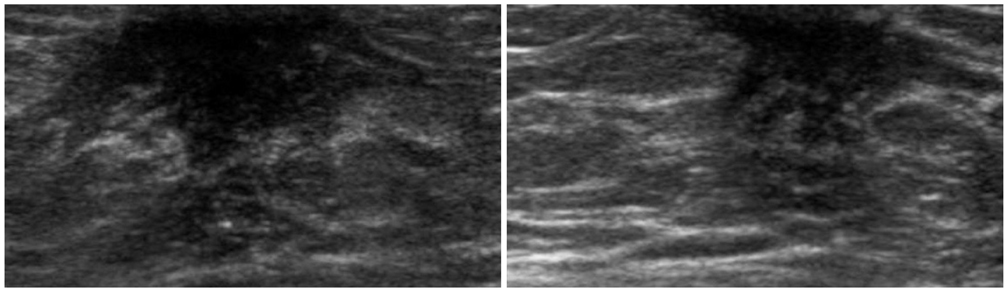
Fig. 3 Bilateral dendritic gynecomastia, 13-year-old boy. Transverse sonogram shows a retroareolar hypoechoic lesion, which may appear irregular finger-like projections at the both breasts.

Fig. 4 Fibroadenoma, 12-year-old girl who presented with right breast lump. Sonogram shows the well-circumscribed oval shaped, iso-to-hypoechoic mass. Histology was fibroadenoma undertaken by ultrasonography guided core biopsy.
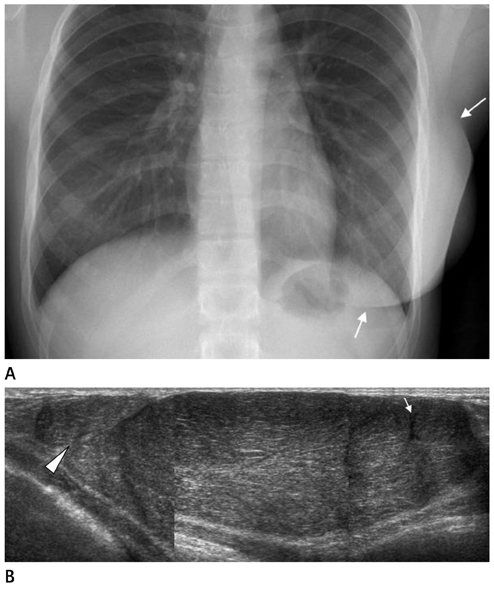
Fig. 5 Juvenile fibroadenoma, 14-year-old girl who presented with asymmetric left breast enlargement. A. Simple chest radiography shows asymmetric huge left breast mass (arrows). B. Sonogram shows the hyperechoic septation (arrowhead) and smaller anechoic cleft (arrow) within a huge, well-circumscribed, fairly uniform hypoechogenic mass. Histology was juvenile fibroadenoma undertaken by excisional biopsy.
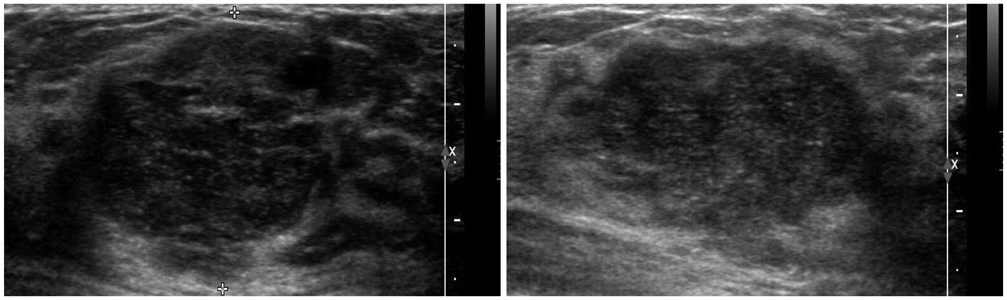
Fig. 6 Cancer in situ with fibroadenoma, 18-year-old girl who presented with left palpable mass. Sonogram shows the round, macrolobulated mass with heterogenous echogenicity. Mammotome biopsy was done. Histology showed a juvenile fibroadenoma with focally irregular border and florid ductal hyperplasia. It was recommended to excise the mass completely. Excision was done 6 months later. Pathologic confirmation was ductal carcinoma in situ with a juvenile fibroadenoma with microcalcification.
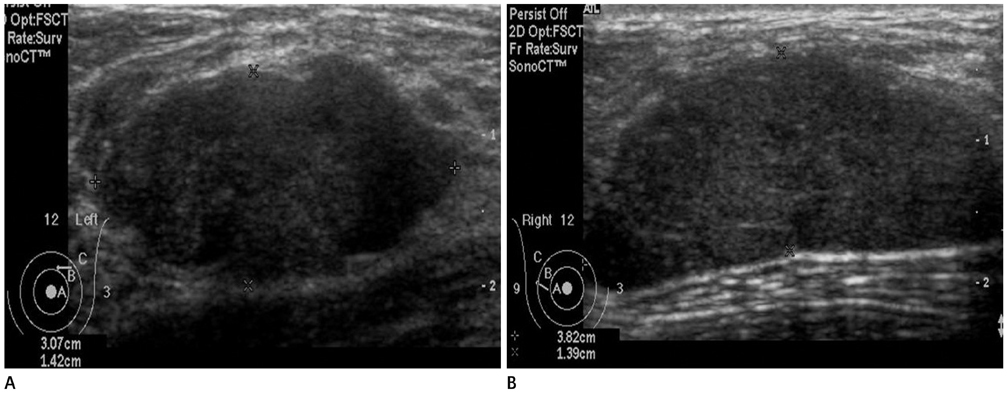
Fig. 7 Benign phyllodes tumor, 15-year-old girl who presented with both rubbery breast masses. A, B. Sonogram shows the well-circumscribed oval shaped, hypoechoic masses at the left (A) and right (B) breast. Sonogram (left and right) are similar to the appearance of a juvenile fibroadenoma. But, histology showed benign phyllodes tumor at the left breast and juvenile fibroadenoma at the right.
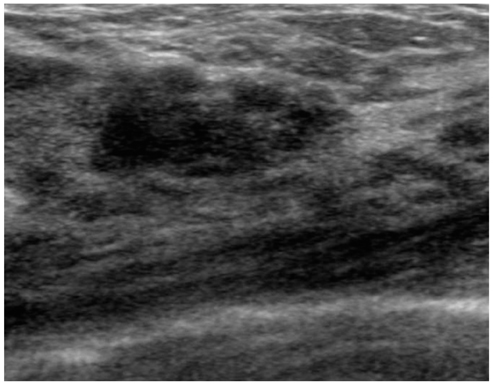
Fig. 8 Fibrocystic change, 17-year-old girl. Sonogram shows a lobulating contoured, well marginated, predominantly hypoechoic mass with some internal echogenic foci.

Fig. 9 Mastitis and abscess, a female baby at postnatal age of 14 days who presented with fever and erythematous breast. A. Sonogram shows a well-circumscribed, ovoid shaped, heterogeneously hypoechoic lesion at the left subareolar area. Needle aspiration was done and S. aureus was found. B. Follow up sonogram shows a markedly decreased extent of the lesion after antibiotic treatment during 50 days.
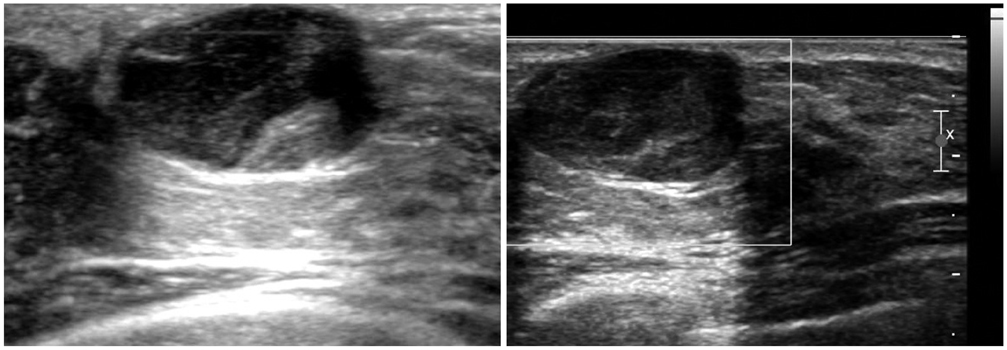
Fig. 10 Epidermoid cyst, 14-year-old girl who presented with a small movable left breast lump. Sonogram shows a well-circumscribed, ovoid shaped, predominantly hypoechoic mass with heterogeneous internal echotexture and no internal vascularity that is superficial in location. Ultrasound-guided core biopsy was undertaken. Histology showed an epidermoid cyst.

Fig. 11 Cystic lymphangioma, 18-year-old boy who presented with swelling of left axilla. A. Chest radiograph shows a asymmetric left axillary swelling (arrows). B, C. Contrast-enhanced CT scan shows a low-attenuated localized lobulating multiseptated cystic mass with septal wall enhancement in the left lateral chest wall and axilla, along the neurovascular bundle. There is no evidence of enhancing solid portion in the mass or no evidence of bony destruction. D, E. Coronal T1-weighted (D) and T2-weighted (E) MR image shows a cystic mass with multiple septa (arrows). Histology showed cystic lymphangioma taken by excisional biopsy.
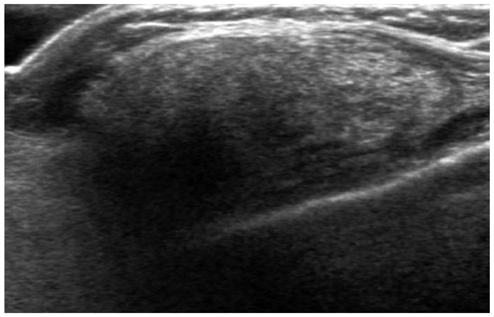
Fig. 12 Fibrolipoma, 6-year-old girl who presented with right breast lump. Sonogram shows the well-circumscribed oval shaped, heterogenous hyperchoic mass.

Fig. 13 Fat necrosis, 16-year-old boy who presented with right chest wall palpable mass after having minor blunt trauma by a soccer ball. A. Sonogram shows an encapsulated, well-circumscribed, beaded shaped, heterogenously isoechoic lesion at the right subareolar area. There is no breast parenchymal tissue. Sonography guided core biopsy (14 G automated gun) was undertaken and histology showed fat necrosis with fibroconnective tissue. B. Color Doppler image shows no internal vascularity with the lesion.
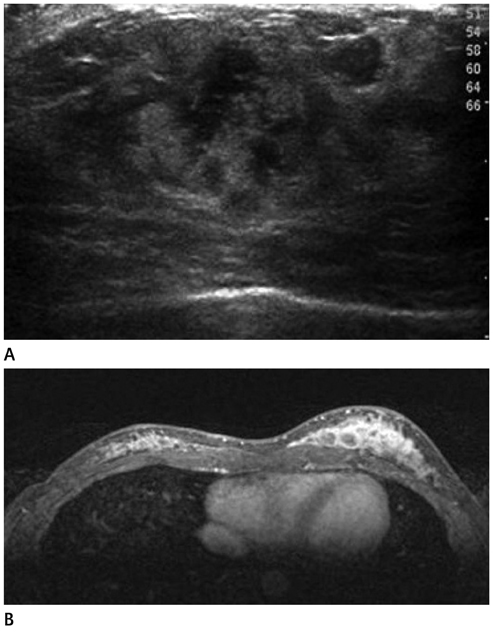
Fig. 14 Rhabdomyosarcoma, 21-year-old women. A. Sonogram shows a huge, irregular shape, indistinct marginated heterogenous hypoechoic mass in left breast lower inner quadrant. B. MR image shows multifocal infiltrating, ill-defined mass with intermediate signal intensity on T1 weighted image and high signal intensity on T2 weighted image (not shown). Post-contrast enhanced MR image shows ring-like enhancing mass with early rapid contrast enhancement and delayed washout. Histology showed embryonal type of rhabdomyosarcoma.
Reference
-
1. Bock K, Duda VF, Hadji P, Ramaswamy A, Schulz-Wendtland R, Klose KJ, et al. Pathologic breast conditions in childhood and adolescence: evaluation by sonographic diagnosis. J Ultrasound Med. 2005. 24:1347–1354. quiz 1356-1357.2. Venta LA, Dudiak CM, Salomon CG, Flisak ME. Sonographic evaluation of the breast. Radiographics. 1994. 14:29–50.3. Siegel MJ. Siegel MJ, editor. Chest. Pediatric sonography. 2002. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins;201–211.4. Chung EM, Cube R, Hall GJ, González C, Stocker JT, Glassman LM. From the archives of the AFIP: breast masses in children and adolescents: radiologic-pathologic correlation. Radiographics. 2009. 29:907–931.5. Kopans DB. Breast Imaging. 1997. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;497–505.6. Stavros AT. Evaluation of the male breast. Breast Ultrasound. 2004. Philadelphia, PA: Lippincott Williams & Wilkins;712–714.7. Yitta S, Singer CI, Toth HB, Mercado CL. Image presentation. Sonographic appearances of benign and malignant male breast disease with mammographic and pathologic correlation. J Ultrasound Med. 2010. 29:931–947.8. Coffin CM. Stocker JT, Dehner LP, editors. The breast. Pediatric pathology. 2002. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;207–208.9. Goel NB, Knight TE, Pandey S, Riddick-Young M, de Paredes ES, Trivedi A. Fibrous lesions of the breast: imaging-pathologic correlation. Radiographics. 2005. 25:1547–1559.10. Rosai J. Rosai J, editor. Breast. Rosai and Ackerman's surgical pathology. 2004. 9th ed. St Louis, MO: Mosby;1769–1773.11. Cole-Beuglet C, Soriano RZ, Kurtz AB, Goldberg BB. Fibroadenoma of the breast: sonomammography correlated with pathology in 122 patients. AJR Am J Roentgenol. 1983. 140:369–375.12. Kronemer KA, Rhee K, Siegel MJ, Sievert L, Hildebolt CF. Gray scale sonography of breast masses in adolescent girls. J Ultrasound Med. 2001. 20:491–496.13. Baker KS, Monsees BS, Diaz NM, Destouet JM, McDivitt RW. Carcinoma within fibroadenomas: mammographic features. Radiology. 1990. 176:371–374.14. Vade A, Lafita VS, Ward KA, Lim-Dunham JE, Bova D. Role of breast sonography in imaging of adolescents with palpable solid breast masses. AJR Am J Roentgenol. 2008. 191:659–663.15. Yilmaz E, Sal S, Lebe B. Differentiation of phyllodes tumors versus fibroadenomas. Acta Radiol. 2002. 43:34–39.16. Liberman L, Bonaccio E, Hamele-Bena D, Abramson AF, Cohen MA, Dershaw DD. Benign and malignant phyllodes tumors: mammographic and sonographic findings. Radiology. 1996. 198:121–124.17. Greydanus DE, Matytsina L, Gains M. Breast disorders in children and adolescents. Prim Care. 2006. 33:455–502.18. Pettinato G, Manivel JC, Kelly DR, Wold LE, Dehner LP. Lesions of the breast in children exclusive of typical fibroadenoma and gynecomastia. A clinicopathologic study of 113 cases. Pathol Annu. 1989. 24(Pt 2):296–328.19. Chantra PK, Tang JT, Stanley TM, Bassett LW. Circumscribed fibrocystic mastopathy with formation of an epidermal cyst. AJR Am J Roentgenol. 1994. 163:831–832.20. Taira N, Aogi K, Ohsumi S, Takashima S, Kawamura S, Nishimura R. Epidermal inclusion cyst of the breast. Breast Cancer. 2007. 14:434–437.21. Crystal P, Shaco-Levy R. Concentric rings within a breast mass on sonography: lamellated keratin in an epidermal inclusion cyst. AJR Am J Roentgenol. 2005. 184:3 Suppl. S47–S48.22. Faul JL, Berry GJ, Colby TV, Ruoss SJ, Walter MB, Rosen GD, et al. Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med. 2000. 161(3 Pt 1):1037–1046.23. Brown LR, Reiman HM, Rosenow EC 3rd, Gloviczki PM, Divertie MB. Intrathoracic lymphangioma. Mayo Clin Proc. 1986. 61:882–892.24. Miyake H, Shiga M, Takaki H, Hata H, Onishi R, Mori H. Mediastinal lymphangiomas in adults: CT findings. J Thorac Imaging. 1996. 11:83–85.25. Weiss S, Goldblum J. Benign lipomatous tumors: Enzinger and Weiss's soft tissue tumors. 2001. 4th ed. St Louis, MO: Mosby;571–639.26. Kransdorf M, Murphey M. Lipomatous tumors. Imaging of soft tissue tumors. 1997. Philadelphia, PA: Saunders;57–101.27. Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. From the archives of the AFIP: benign musculoskeletal lipomatous lesions. Radiographics. 2004. 24:1433–1466.28. Hogge JP, Robinson RE, Magnant CM, Zuurbier RA. The mammographic spectrum of fat necrosis of the breast. Radiographics. 1995. 15:1347–1356.29. Soo MS, Kornguth PJ, Hertzberg BS. Fat necrosis in the breast: sonographic features. Radiology. 1998. 206:261–269.30. Sakorafas GH, Tsiotou AG. Ductal carcinoma in situ (DCIS) of the breast: evolving perspectives. Cancer Treat Rev. 2000. 26:103–125.31. Moon WK, Myung JS, Lee YJ, Park IA, Noh DY, Im JG. US of ductal carcinoma in situ. Radiographics. 2002. 22:269–280. discussion 280-281.32. Agrons GA, Wagner BJ, Lonergan GJ, Dickey GE, Kaufman MS. From the archives of the AFIP. Genitourinary rhabdomyosarcoma in children: radiologic-pathologic correlation. Radiographics. 1997. 17:919–937.33. Yang WT, Muttarak M, Ho LW. Nonmammary malignancies of the breast: ultrasound, CT, and MRI. Semin Ultrasound CT MR. 2000. 21:375–394.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breast lesions during pregnancy and lactation: a pictorial essay
- Unexpected hyperechoic lesions of the breast and their correlations with pathology: a pictorial essay
- Ultrasonography of Various Thyroid Diseases in Children and Adolescents: A Pictorial Essay
- National Patterns and Characteristics in Pediatric Dental Emergency Visits for Dental Conditions
- Vestibular migraine of childhood
