Report of 1,000 Kidney Transplants at the Sungkyunkwan University of Korea
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kmhyj111@skku.edu
- KMID: 2097081
- DOI: http://doi.org/10.4285/jkstn.2009.23.2.141
Abstract
- BACKGROUND
This study aims to report clinical outcome and long term graft and patient survival rate of one thousand kidney transplantation. We analyzed risk factors that impact on graft survival in the 1,000 case of kidney transplantation through this study.
METHODS
We have performed 1,000 cases of kidney transplantation in Samsung Medical Center, Seoul, Korea from February 1995 to January 2008. We retrospectively reviewed medical record of recipients and donors.
RESULTS
The mean follow up period was 69 months. Composition of type of donor was living donor, 653 cases and deceased donor, 347 cases. Type of donor source was mostly living-related type. 94 cases had graft failure. Major cause of graft failure was chronic allograft nephropathy. And major viral infection was cytomegalovirus infection. Major non-viral infection was urinary tract infection. 47 cases of immediate post operative complication was diagnosed as lymphocele. Overall 10-year graft survival rate was 83.9% respectively. 10-year patient survival rate was 95.7% respectively. 10-year graft survival and patient survival of recipient were significantly different between living donation group and deceased donation group.
CONCLUSIONS
In this report, only two risk factor were statically significant difference.
Keyword
MeSH Terms
Figure
-
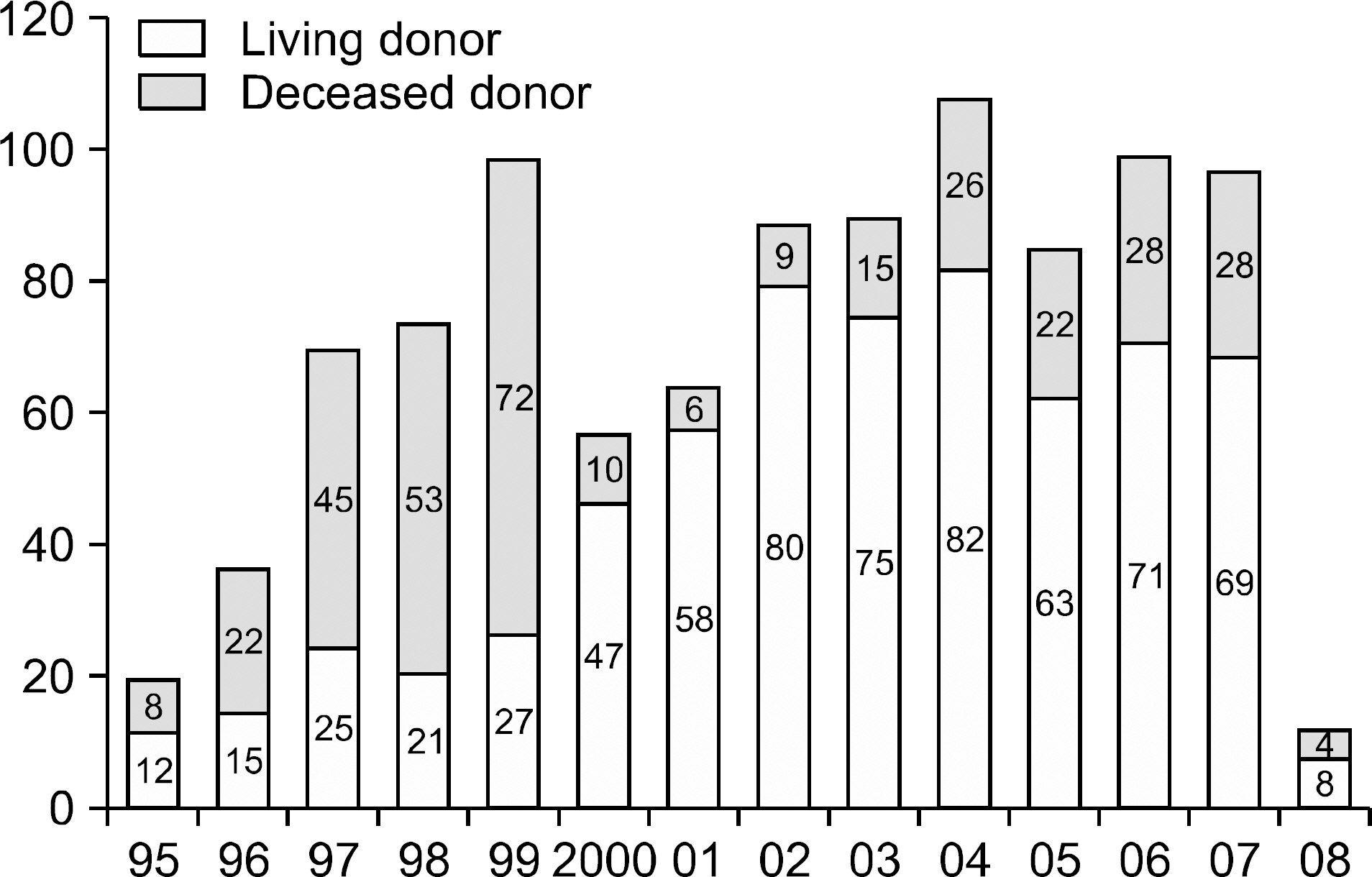
Fig. 1. Number of kidney transplantation from 1995 to 2008.
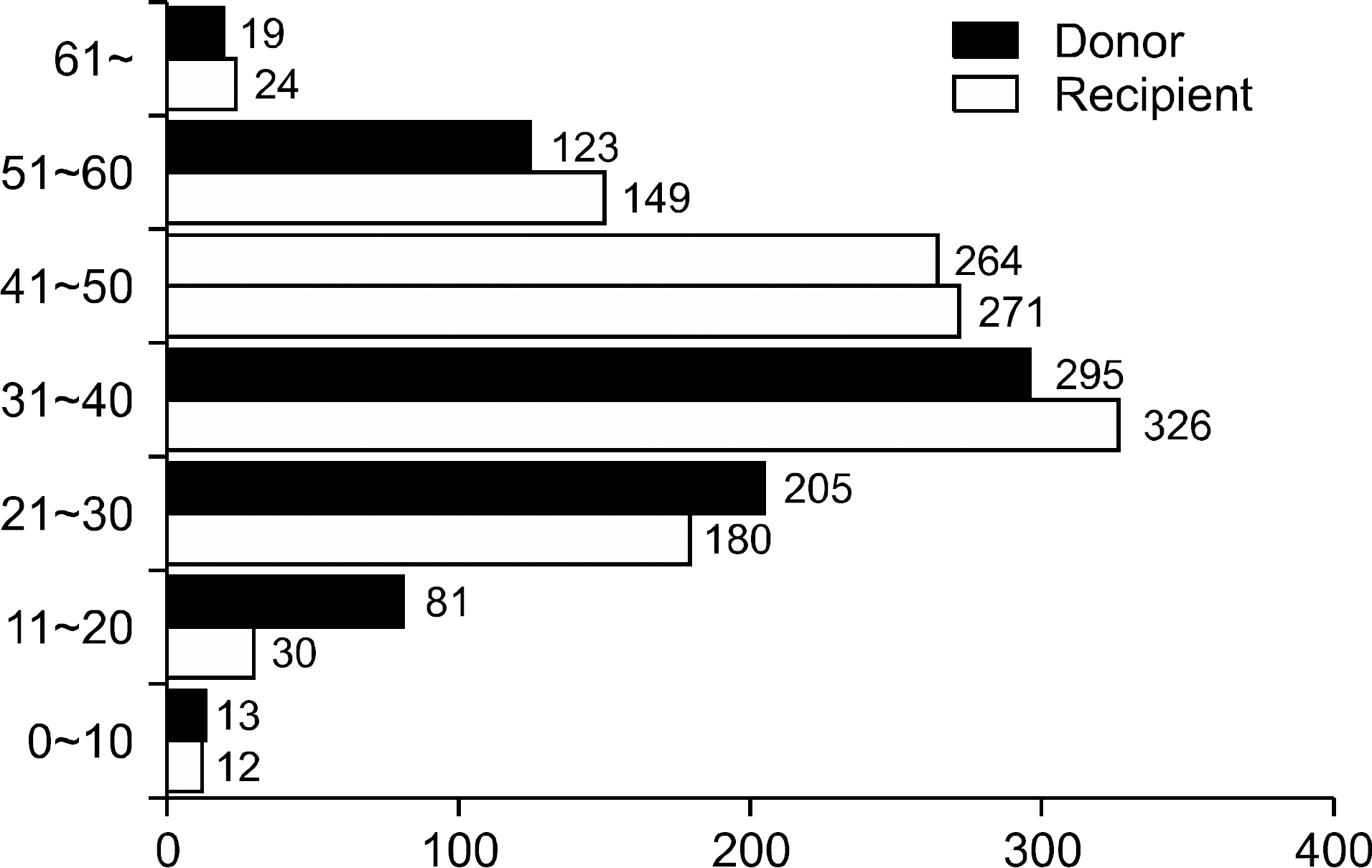
Fig. 2. Distribution of age in recipients and donors.
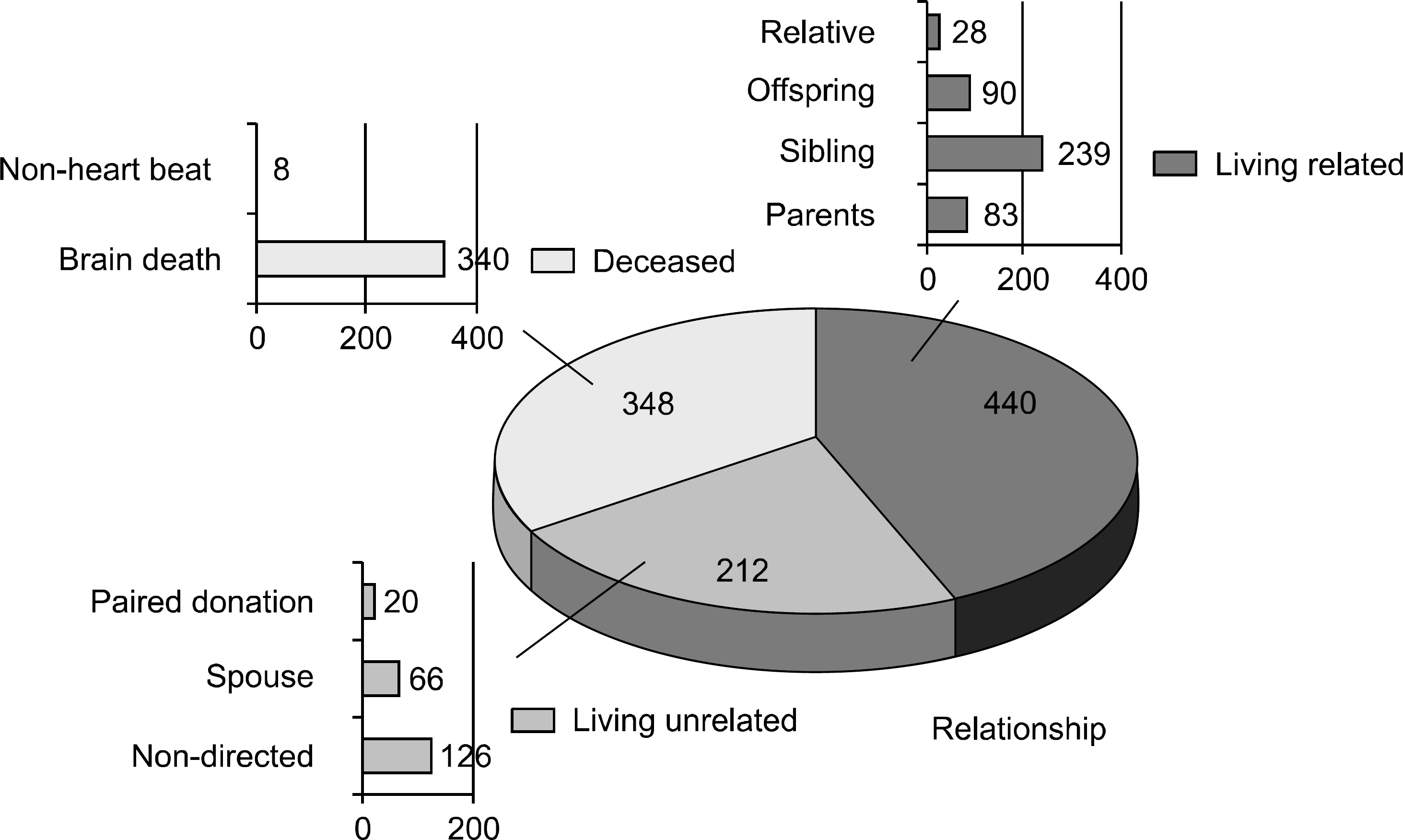
Fig. 3. Relationships of donor and recipient.
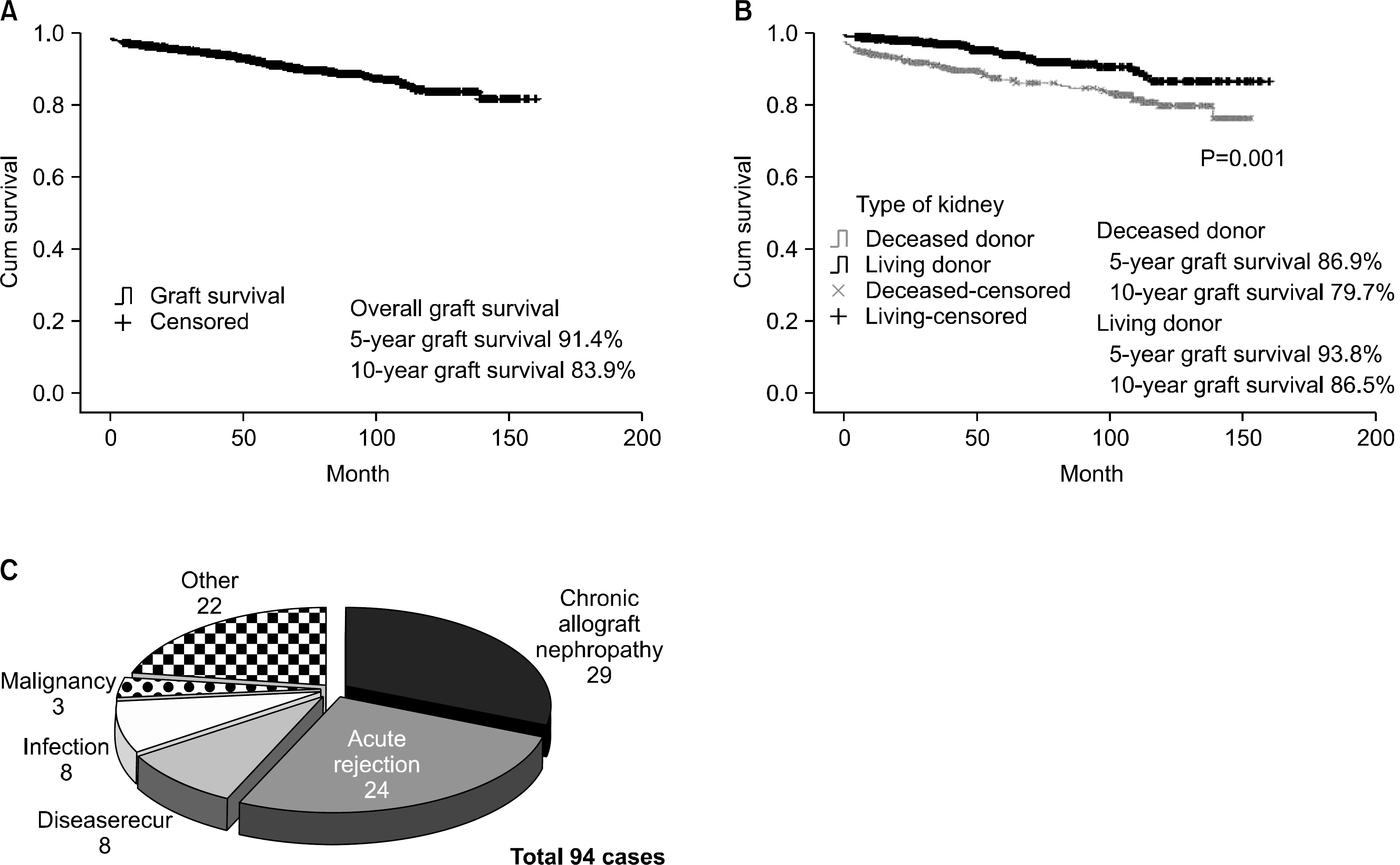
Fig. 4. (A) Overall graft survival, (B) Graft survival according to type of donor, (C) Causes of graft failure.
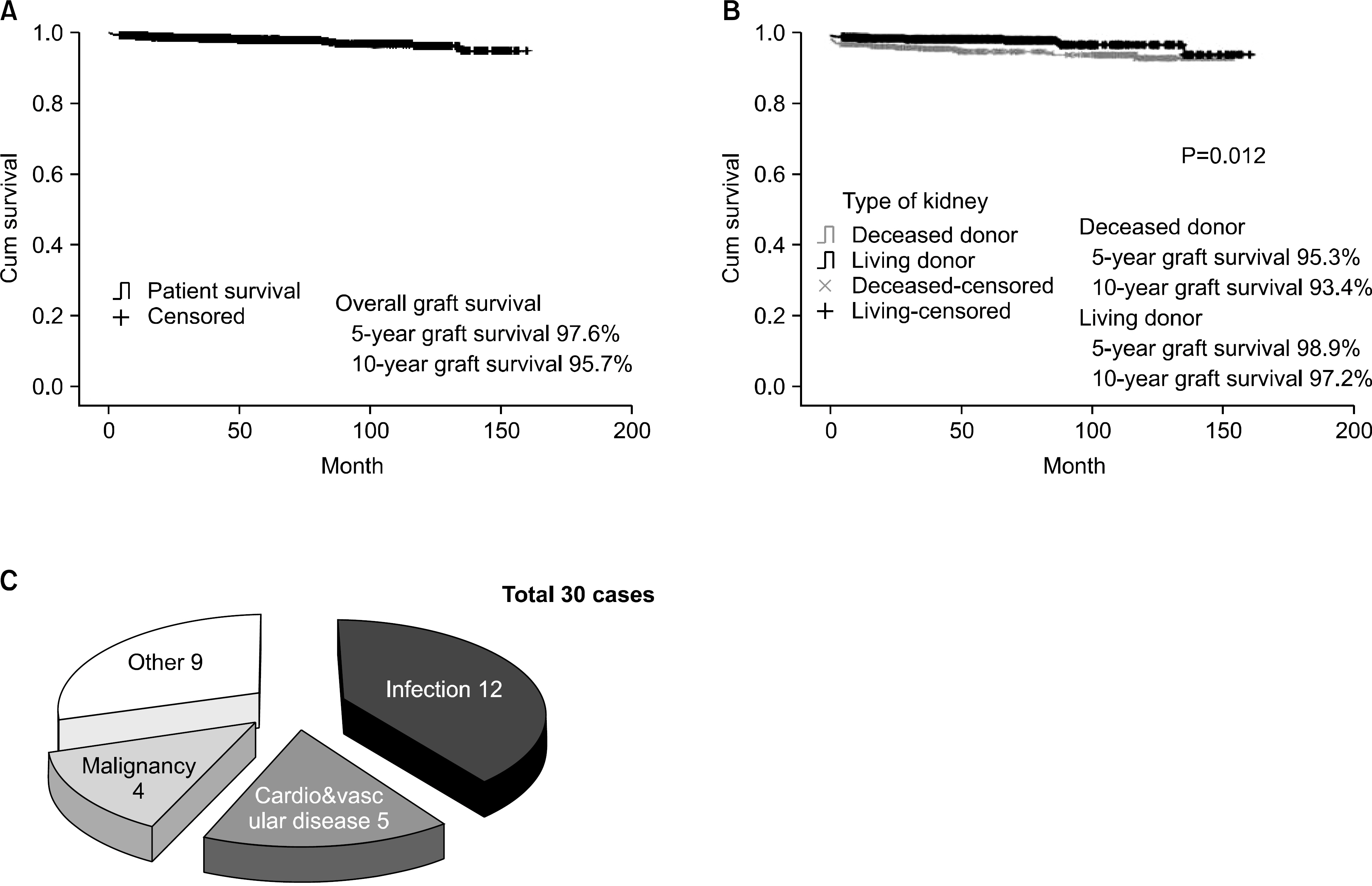
Fig. 5. (A) Overall patient survival, (B) Patients survival according to type of donor, (C) Causes of patient death.
Cited by 2 articles
-
Analysis of 1,500 Kidney Transplantations at Sungkyunkwan University
Jae Woong Hong, Milljae Shin, Hyung Hwan Moon, Sanghoon Lee, Jong Man Kim, Jae Berm Park, Choon Hyuck David Kwon, Jae-Won Joh, Suk-Koo Lee, Sung-Joo Kim
J Korean Soc Transplant. 2014;28(1):25-35. doi: 10.4285/jkstn.2014.28.1.25.Actual 10-year Outcomes of Tacrolimus/MMF Compared with Cyclosporin/MMF in Kidney Transplantation
Yaerim Kim, Sungbae Park, Hyoungtae Kim, Seungyeup Han
J Korean Soc Transplant. 2014;28(2):69-77. doi: 10.4285/jkstn.2014.28.2.69.
Reference
-
1). Kim JY, Kim SH, Kim YS, Choi BS, Kim JC, Park SC, et al. Report of 1,500 Kidney Transplants at the Catholic University of Korea. J Korean Soc Transplant. 2006; 20:172–80.2). Sirinivas TR, Meier-Kriesche HU. Minimizing immuno-suppression, an alternative approach to reducing side effects: objectives and interim result. Clin J Am Soc Nephrol. 2008; 3(S2):S101–16.3). Ekberg H, Tedesco-Silva H, Demirbas A, Vítko S, Nashan B, Gürkan A, et al. ELITE- Symphony Study. Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med. 2007; 375:2562–75.4). Taber DJ, Weimert NA, Henderson F, Lin A, Bratton CF, Chavin KD, et al. Long-term efficacy of induction therapy with anti-interleukin-2 receptor antibodies or thymoglobulin compared with no induction therapy in renal transplantation. Transplant Proc. 2008; 40:3401–7.
Article5). Korean Network for Organ Sharing(KONOS). KONOS annual report, 2008 [Internet] Seoul: KONOS, 2009. Available from. http://www.konos.go.kr.6). Meng HL, Jin XB, Li XT, Wang HW, Lü JJ. Impact of human leukocyte antigen matching and recipients’ panel reactive antibodies on two-year outcome in presensitized renal allograft recipients. Chin Med J(Engl). 2009; 122:420–6.7). Süsal C, Opelz G. Kidney graft failure and presensitiza-tion against HLA class I and class II antigens. Transplantation. 2002; 73:1269–73.8). El-Zoghby ZM, Stegall MD, Lager DJ, Kremers WK, Amer H, Gloor JM, et al. Identifying specific causes of kidney allograft loss. Am J Transplant. 2009; 9:527–35.
Article9). Sagedal S, Hartmann A, Rollag H. The impact of early cytomegalovirus infection and disease in renal transplant recipients. Clin Microbiol Infect. 2005; 11:518–30.
Article10). Bonvoisin C, Weekers L, Xhiqnesse P, Grosch S, Milicevic M, Krzesinski JM. Polyomavirus in renal transplantation: a hot problem. Transplantation. 2008; 85(S):S42–8.
Article11). Trofe J, Hirsch HH, Ramos E. Polyomavirus-associated nephropathy: upate of clinical management in kidney transplant patients. Transpl Infect Dis. 2006; 8:76–85.12). Domhan S, Zeier M, Abdollahi A. Immunosuppressive therapy and posttransplant malignancy. Nephrol Dial Transplant. 2009; 24:1097–103.
Article13). Navarro MD, López-Andréu M, Rodríguez-Benot A, Agüera ML, Del Castillo D, Aljama P. Cancer incidence and survival in kidney transplant patients. Transplant Proc. 2008; 40:2936–40.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Does the timing of acute rejection matter with the graft outcome in kidney transplantation?
- Long-term effects of HLA matching on graft survivals in cyclosporine treated living kidney transplants
- Simultaneous Liver, Kidney Transplantation: A Single Center Experience
- Virtual crossmatch versus complement-dependent cytotoxicity crossmatch in deceased kidney paired donations: a single-center experience from India
- Case Report of Left Retrocaval Ureter: Pre-Transplant CT Urographic Findings and Post-Transplant Outcomes
