Discrepant Bowel Perforation from a Primary Lesion after Chemotherapy of Diffuse Large B Cell Lymphoma
- Affiliations
-
- 1Division of Gastoenterologic Surgery, Department of Surgery, Chonnam National University Medical School, Gwangju, Korea. dockim@chonnam.ac.kr
- KMID: 2040607
- DOI: http://doi.org/10.4174/jkss.2009.76.1.61
Abstract
- Diffuse large B cell lymphoma is the most common type of non-Hodgkin's lymphoma, representing approximately one-third of all cases and involving the gastrointestinal tract in about 18%. With the development of modern chemotherapeutic regimens and advances in medical care, the prognosis for malignant lymphoma can be excellent. However, because of the aggressive adjuvant therapy required, complications such as bowel perforation may be fatal. In cases of chemotherapy for malignant lymphoma, we should keep in mind the possibility of perforation of the bowel after chemotherapy. Early detection is important to save patients.
Figure
-
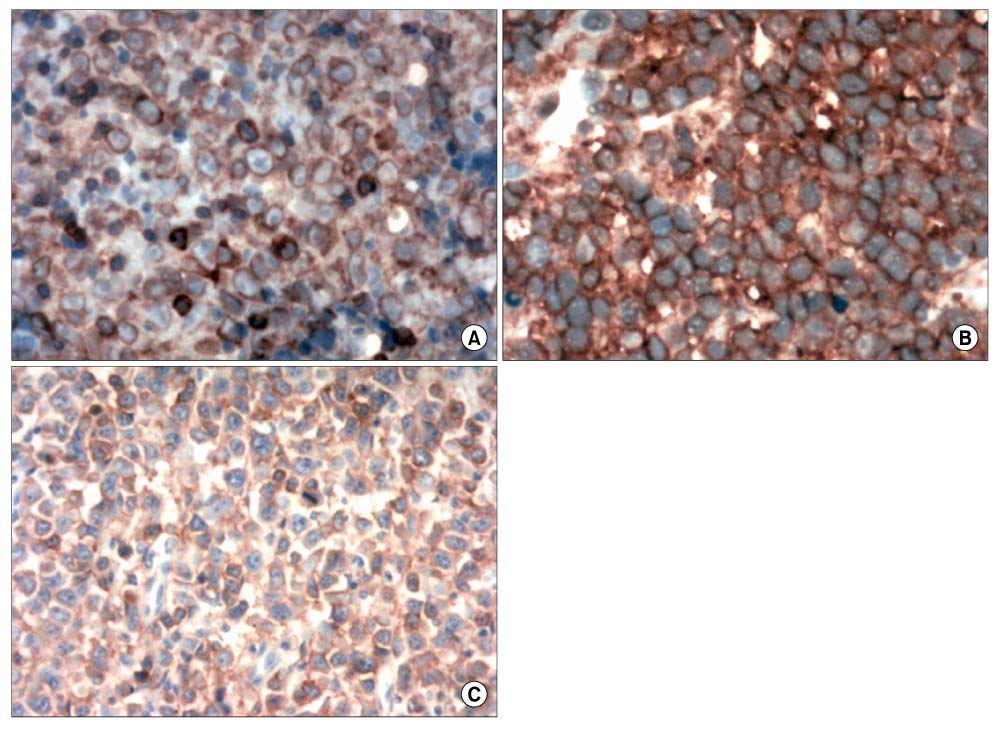
Fig. 1 Immunohistochemical staining for CD 79. There were large nuclei in each case. Tonsil (A), Terminal ileum (B), Intra-abdominal mass (C)(Immunohistochemical staining, ×400).
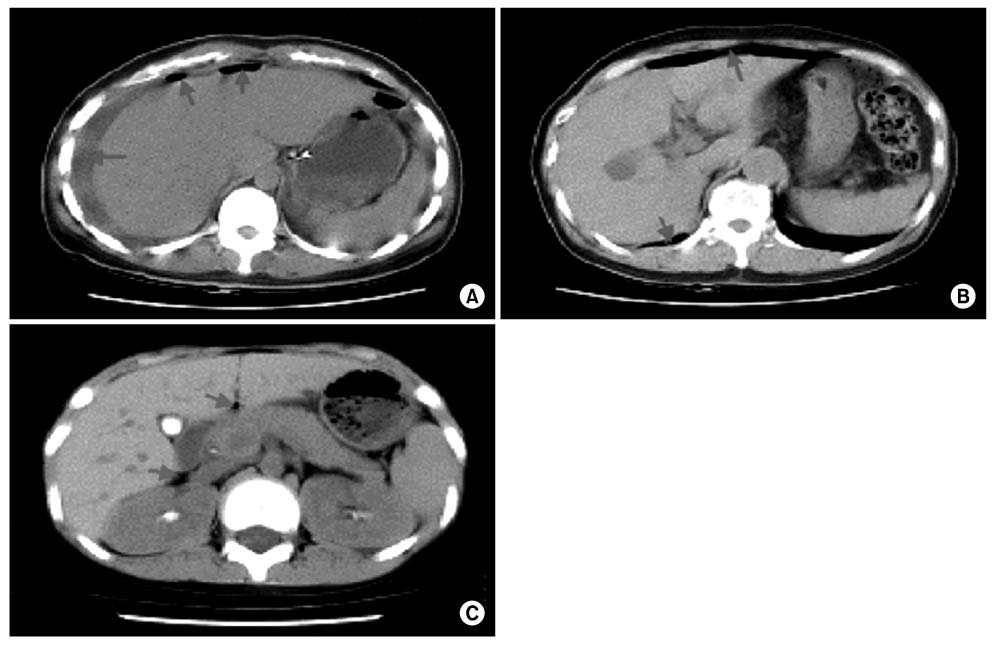
Fig. 2 Abdominal computed tomography. A large amount of fluid and free air (arrow) in the peritoneal cavity (A). Multiple pockets of free air were present in the peritoneal cavity and Morrison's pouch (B). A small area of free air was present around the porta hepatis (C).
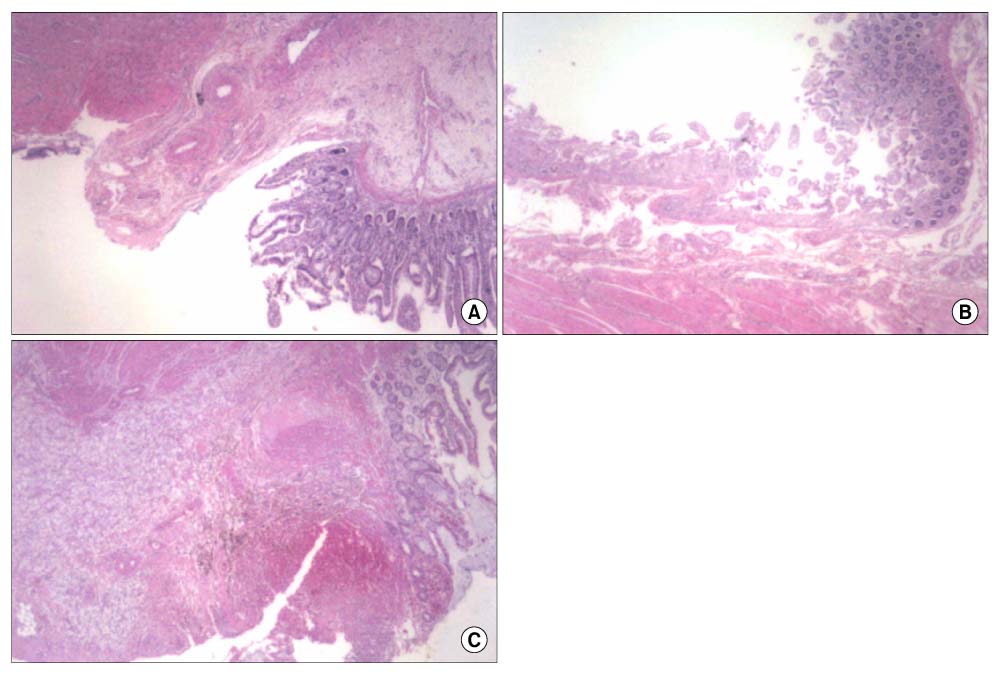
Fig. 3 The area of perforated bowel. Mild mucosal destruction with an irregular surface, intense inflammatory cell infiltration, and perforation (A). The bowel showed mucosal ischemic changes and submucosal edema, with hemorrhage and serosal inflammation (B). The specimen contained many foamy macrophages and multinucleated giant cells in the submucosa and muscle proper, with serosal reaction and a focal segment of mucosal ulceration (C)(H&E, ×20).
Reference
-
1. Hiddemann W. Non-Hodgkin's lymphomas--current status of therapy and future perspectives. Eur J Cancer. 1995. 31:2141–2145.2. James OA, Dan LL. Malignancies of Lymphoid Cells. Harrison's Principles of Internal Medicine. 2001. 15th ed. New York: McGraw-Hill;715–727.3. Fu YS, Perzin KH. Lymphosarcoma of the small intestine. A clinicopathologic study. Cancer. 1972. 29:645–659.4. Sakakura C, Hagiwara A, Nakanishi M, Yasuoka R, Shirasu M, Togawa T, et al. Bowel perforation during chemotherapy for non-hodgkin's lymphoma. Hepatogastroenterology. 1999. 46:3175–3177.5. Libicher M, Lamade W, Kasperk C, Grenacher L, Kauffmann GW. Cicatricial small intestinal stenosis following chemotherapy for a gastrointestinal lymphoma. Dtsch Med Wochenschr. 1996. 121:1359–1362.6. Lundy J, Sherlock P, Kurtz R, Fortner JG, Turnbull AD. Spontaneous perforation of the gastrointestinal tract in patients with cancer. Am J Gastroenterol. 1975. 63:447–450.7. Meyers PA, Potter VP, Wollner N, Exelby P. Bowel perforation during initial treatment for childhood non-Hodgkin's lymphoma. Cancer. 1985. 56:259–261.8. Sherlock P, Oropezar . Jejunal perforations in lymphoma after chemotherapy. Arch Intern Med. 1962. 110:102–107.9. Jones GT, Abramson N. Gastrointestinal necrosis in acute leukemia: a complication of induction therapy. Cancer Invest. 1983. 1:315–320.10. Yuen JS, Chow PK, Ahmed Q. Metastatic lung cancer causing bowel perforations: spontaneous or chemotherapy-related? ANZ J Surg. 2002. 72:245–246.11. Beck JC, Browne JS, Johnson LG. Occurrence of peritonitis during ACTH administration. Can Med Assoc J. 1950. 62:423–426.12. Glenn F, Grafe WR Jr. Surgical complications of adrenal steroid therapy. Ann Surg. 1967. 65:1023–1032.13. Rigotti P, Van Buren CT, Payne WD, Peters C, Kahan BD. Gastrointestinal perforations in renal transplant recipients immunosuppressed with cyclosporin. World J Surg. 1986. 10:137–141.14. Greenstein AJ, Sachar DB, Mann D, Lachman P, Heimann T, Aufses AH Jr. Spontaneous free perforation and perforated abscess in 30 patients with Crohn's disease. Ann Surg. 1987. 205:72–76.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relapse of Ocular Lymphoma following Primary Testicular Diffuse Large B-cell Lymphoma
- Experience of serious intestinal hemorrhage and perforation in small bowel lymphoma: a case report
- A Case of Small Bowel Diffuse Large B-cell Lymphoma Mimicking Crohn's Disease
- A Case of Primary Rectal Diffuse Large B Cell LymphomaPresented as Multiple Polypoid Lesions
- A Case of a Rapidly Progressive Small Bowel Lymphoma with High Ki-67 Expression
