Acute Hyperammonemic Encephalopathy with Features on Diffusion-Weighted Images: Report of Two Cases
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Daejeon, Korea. midosyu@eulji.ac.kr
- KMID: 2002810
- DOI: http://doi.org/10.3348/jksr.2015.72.2.131
Abstract
- Acute hyperammonemic encephalopathy is a rare toxic encephalopathy caused by accumulated plasma ammonia. A few literatures are reported about MRI findings of acute hyperammonemic encephalopathy. It is different from the well-known chronic hepatic encephalopathy. The clinical symptom and MRI findings of acute hyperammonemic encephalopathy can be reversible with proper treatment. Acute hepatic encephalopathy involves the cingulate cortex, diffuse cerebral cortices, insula, bilateral thalami on diffusion-weighted imaging (DWI), and fluid-attenuated inversion-recovery. Acute hepatic encephalopathy might mimic hypoxic-ischemic encephalopathy because of their similar predominant involving sites. We experienced 2 cases of acute hyperammonemic encephalopathy consecutively. They showed restricted diffusion at the cingulate cortex, cerebral cortices, insula, and bilateral dorsomedial thalami on DWI. One patient underwent acute fulminant hepatitis A, the other patient with underlying chronic liver disease had acute liver failure due to hepatotoxicity of tuberculosis medication. In this report, we presented the characteristic features of DWI in acute hyperammonemic encephalopathy. In addition, we reviewed articles on MRI findings of acute hyperammonemic encephalopathy.
MeSH Terms
Figure
-
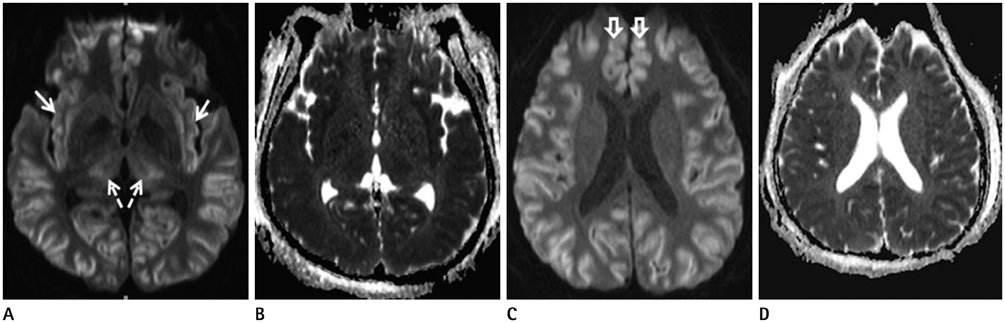
Fig. 1 A 56-year-old male patient with underlying chronic liver disease and newly developed acute hyperammonemic encephalopathy due to tuberculosis medicine. Diffusion-weighted imaging (A, C) shows high signal intensities at both temporo-fronto-parieto-occipial cortices, insula (white solid arrows) (A), cingulate cortex (open arrows) (C) and dorsomedial thalami (dashed arrows) (A). It is confirmed to have reduced diffusion on apparent diffusion coefficient maps (B, D).

Fig. 2 A 47-year-old male patient with acute hyperammonemic encephalopathy due to acute hepatitis A. The diffusion-weighted imaging (A, C), apparent diffusion coefficient map (B, D) show diffusion restriction at insula (white solid arrows) (A), cingulate cortex (open arrows) (C), diffuse cerebral cortices, and bilateral dorsomedial thalami (dashed arrows) (A).
Reference
-
1. Rosario M, McMahon K, Finelli PF. Diffusion-weighted imaging in acute hyperammonemic encephalopathy. Neurohospitalist. 2013; 3:125–130.2. U-King-Im JM, Yu E, Bartlett E, Soobrah R, Kucharczyk W. Acute hyperammonemic encephalopathy in adults: imaging findings. AJNR Am J Neuroradiol. 2011; 32:413–418.3. McKinney AM, Lohman BD, Sarikaya B, Uhlmann E, Spanbauer J, Singewald T, et al. Acute hepatic encephalopathy: diffusion-weighted and fluid-attenuated inversion recovery findings, and correlation with plasma ammonia level and clinical outcome. AJNR Am J Neuroradiol. 2010; 31:1471–1479.4. Choi JM, Kim YH, Roh SY. Acute hepatic encephalopathy presenting as cortical laminar necrosis: case report. Korean J Radiol. 2013; 14:324–328.5. Prakash R, Mullen KD. Mechanisms, diagnosis and management of hepatic encephalopathy. Nat Rev Gastroenterol Hepatol. 2010; 7:515–525.6. Paller KA, Acharya A, Richardson BC, Plaisant O, Shimamura AP, Reed BR, et al. Functional Neuroimaging of Cortical Dysfunction in Alcoholic Korsakoff's Syndrome. J Cogn Neurosci. 1997; 9:277–293.7. Wadzinski J, Franks R, Roane D, Bayard M. Valproate-associated hyperammonemic encephalopathy. J Am Board Fam Med. 2007; 20:499–502.8. Sharma P, Eesa M, Scott JN. Toxic and acquired metabolic encephalopathies: MRI appearance. AJR Am J Roentgenol. 2009; 193:879–886.9. Arnold SM, Els T, Spreer J, Schumacher M. Acute hepatic encephalopathy with diffuse cortical lesions. Neuroradiology. 2001; 43:551–554.10. Bindu PS, Sinha S, Taly AB, Christopher R, Kovoor JM. Cranial MRI in acute hyperammonemic encephalopathy. Pediatr Neurol. 2009; 41:139–142.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diffusion Weighted Magnetic Resonance Imaging in a Patient with Acute Wernicke Encephalopathy
- Two Cases of Hypertensive Brainstem Encephalopathy
- Reversible Splenial Lesion Syndrome Associated with Encephalitis/Encephalopathy Improved with Short-Term Steroid Treatment
- Reversible Burst-suppression Pattern of Acute Hyperammonemic Encephalopathy
- Uremic Encephalopathy with Atypical Magnetic Resonance Features on Diffusion-Weighted Images
