Multivariate Analysis of the Prognostic Significance of Resection Weight after Transurethral Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer
- Affiliations
-
- 1Department of Urology, Yeungnam University College of Medicine, Daegu, Korea. htkim@ynu.ac.kr
- KMID: 1988755
- DOI: http://doi.org/10.4111/kju.2012.53.7.457
Abstract
- PURPOSE
Tumor size and multiplicity are known to be important prognostic factors in non-muscle-invasive bladder cancer (NMIBC). However, evaluation of accurate tumor size is subjective and difficult. Furthermore, there are limitations to the objectification of tumor volume in the case of multiple lesions. In this study, we investigated the relation between resection weight after transurethral resection of bladder tumor (TURBT) and the prognosis of NMIBC.
MATERIALS AND METHODS
This was a retrospective analysis of 406 patients diagnosed with pTa or pT1 bladder tumors after TURBT between September 1999 and May 2010. The patient's age, sex, underlying diseases, cancer stage, grade, multiplicity, tumor size, lymphovascular invasion, and resection weight were analyzed in relation to cancer progression and recurrence. The resection weight was weighted after formaldehyde fixation.
RESULTS
The mean follow-up time was 76.9 months (range, 12 to 167 months) in 406 patients diagnosed as having NMIBC. Mean resection weight was 4.5 g (range, 0.1 to 35.0 g). The cancer recurred in 99 patients (24.4%), and disease progression was noted in 30 patients (7.4%). Resection weight was categorized as greater than or less than 2 g by use of receiver operator characteristic curves. Cancer grade (p=0.022) and multiplicity (p=0.043) were significantly related to cancer recurrence in the analysis with Cox's multivariate proportional hazard model. Cancer grade (p=0.001) and resection weight (p=0.018) were related to disease progression.
CONCLUSIONS
Resection weight after TURBT was significantly related to progression of NMIBC. Resection weight was an independent factor of progression. Further management should be considered if the resection weight exceeds 2 g.
Keyword
MeSH Terms
Figure
-
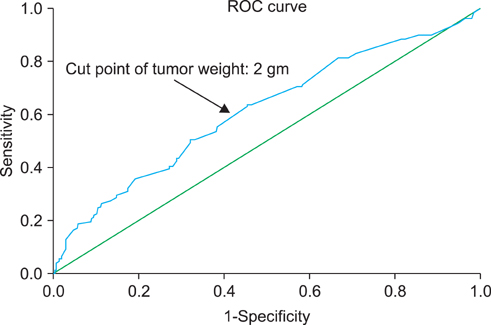
FIG. 1 Receiver-operating characteristic (ROC) curve (tumor weight). Points (black arrow) on the ROC curve represent the possibility levels generated from the logistic regression analysis that was used to select the optimal cutoff point. A predicted probability of 2 provided a sensitivity of 70.5% and a specificity of 57.0%.
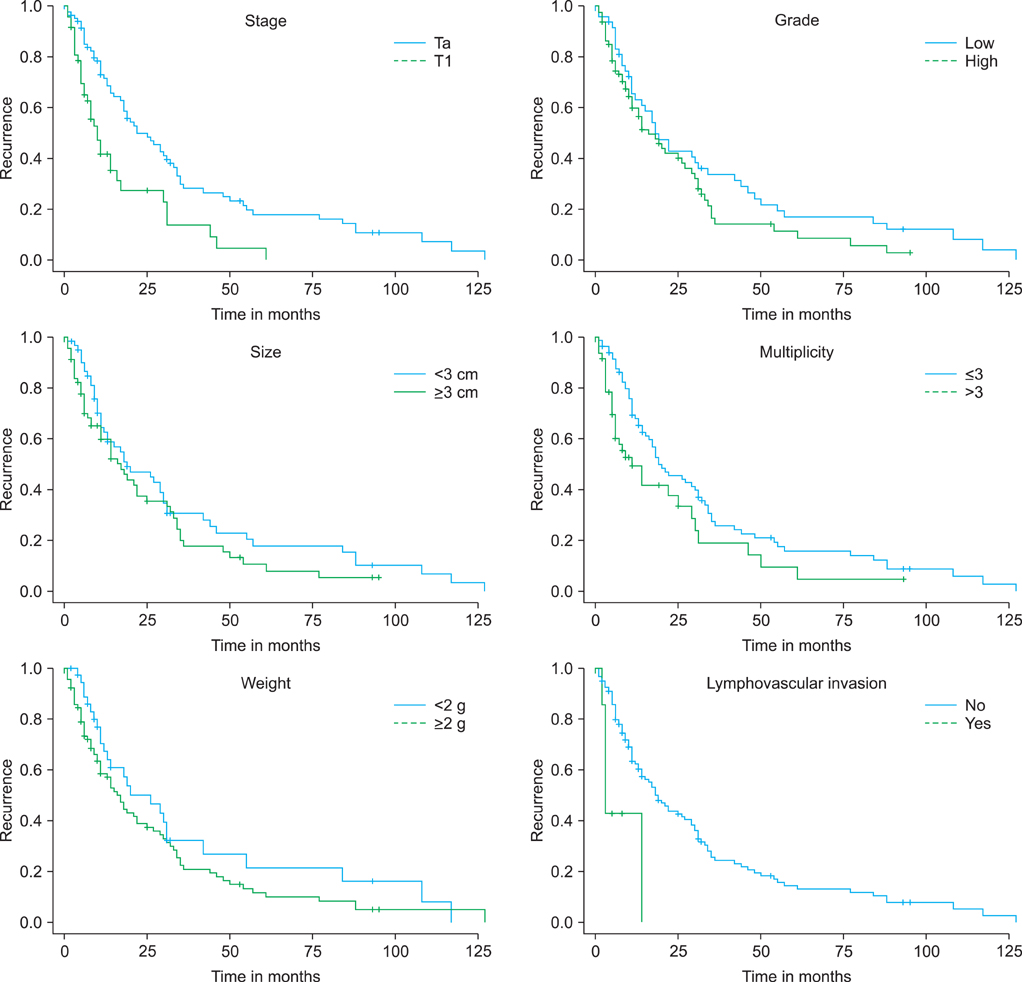
FIG. 2 Kaplan-Meier plot for recurrence comparing Ta and T1 tumors (p=0.001), grades low and high (p=0.125), tumors greater than and less than 3 cm (p=0.190), multiplicity more than 3 and less than 3 (p=0.024), tumors greater than and less than 2 g (p=0.184), and lymphovascular invasion (p=0.002).
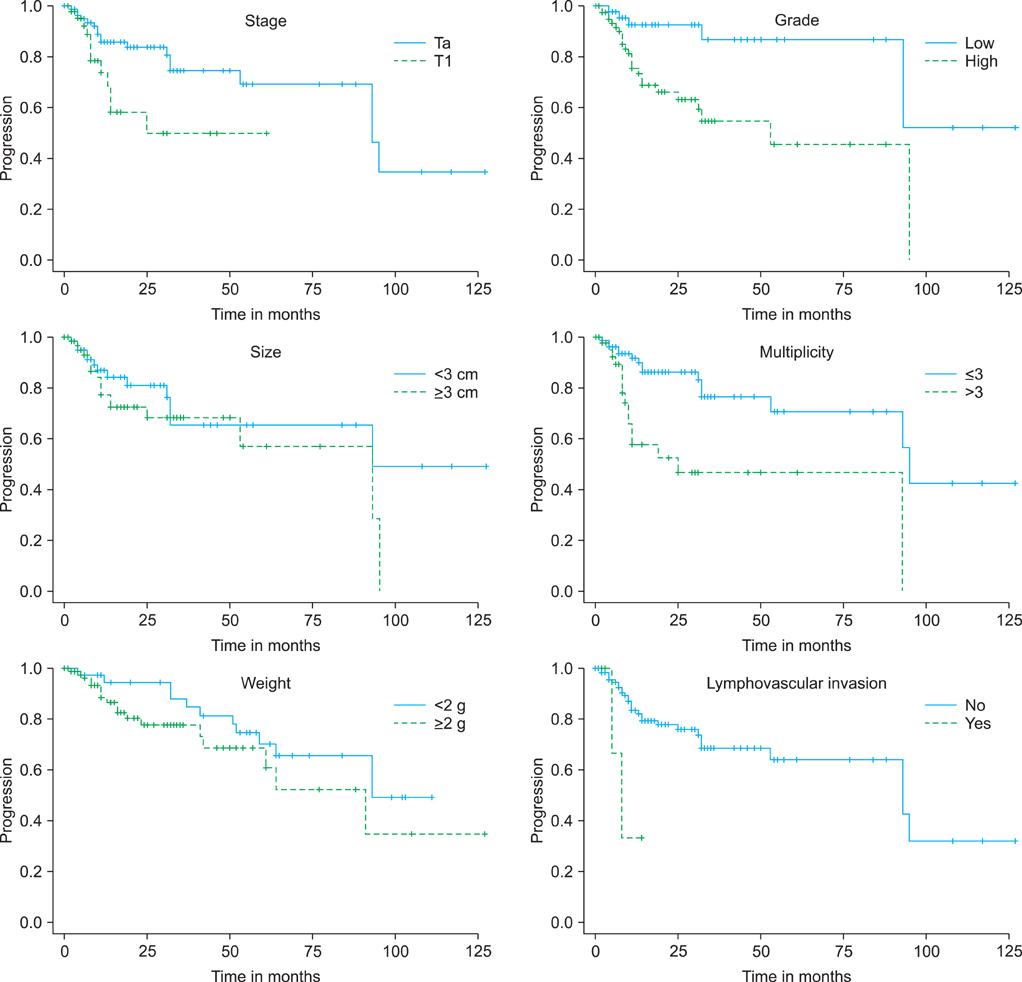
FIG. 3 Kaplan-Meier plot for progression comparing Ta and T1 tumors (p=0.013), grades low and high (p=0.002), tumors greater than and less than 3 cm (p=0.166), multiplicity more than 3 and less than 3 (p=0.001), tumors greater than and less than 2 g (p=0.017), and lymphovascular invasion (p=0.023).
Reference
-
1. National Cancer Center [internet]. The statistics report: the incidence of cancer on 2003-2005 and the survival rate on 1993-2005. c2012. cited 2009 Apr 1. Goyang: National Cancer Center;Available from: http://www.ncc.re.kr.2. Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al. Cancer statistics, 2005. CA Cancer J Clin. 2005. 55:10–30.3. Kim YJ, Moon KH, Kim KR, Kim CS. Significance of T1 substaging on the recurrence and progression of bladder cancer. Korean J Urol. 2000. 41:1323–1328.4. Kwon S, Park CM, Kim HG, Gang GH, Song JS, Park JY. Prognostic significance of the tumor configuration in superficial bladder tumor. Korean J Urol. 2006. 47:237–243.5. Reading J, Hall RR, Parmar MK. The application of a prognostic factor analysis for Ta.T1 bladder cancer in routine urological practice. Br J Urol. 1995. 75:604–607.6. Hall MC, Chang SS, Dalbagni G, Pruthi RS, Seigne JD, Skinner EC, et al. Guideline for the management of nonmuscle invasive bladder cancer (stages Ta, T1, and Tis): 2007 update. J Urol. 2007. 178:2314–2330.7. Legrand G, Soliman H, Dubosq F, Verine J, Desgrandchamps F, de The H, et al. Prevalence and spectrum of microsatellite alterations in nonmuscle invasive bladder cancers. Am J Cancer Res. 2011. 1:595–603.8. Kurth KH, Denis L, Bouffioux C, Sylvester R, Debruyne FM, Pavone-Macaluso M, et al. Factors affecting recurrence and progression in superficial bladder tumours. Eur J Cancer. 1995. 31A:1840–1846.9. Millan-Rodriguez F, Chechile-Toniolo G, Salvador-Bayarri J, Palou J, Vicente-Rodriguez J. Multivariate analysis of the prognostic factors of primary superficial bladder cancer. J Urol. 2000. 163:73–78.10. Ali-El-Dein B, Sarhan O, Hinev A, Ibrahiem el-HI, Nabeeh A, Ghoneim MA. Superficial bladder tumours: analysis of prognostic factors and construction of a predictive index. BJU Int. 2003. 92:393–399.11. Sylvester RJ, van der Meijden AP, Oosterlinck W, Witjes JA, Bouffioux C, Denis L, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006. 49:466–475.12. Barocas DA, Clark PE. Bladder cancer. Curr Opin Oncol. 2008. 20:307–314.13. Hirao Y, Kim WJ, Fujimoto K. Environmental factors promoting bladder cancer. Curr Opin Urol. 2009. 19:494–499.14. Jones JS, Larchian WA. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Non-muscle-invasive bladder cancer (Ta, T1, and CIS). Campbell-Walsh urology. 2012. 10th ed. Philadelphia: Saunders;2335–2354.15. Kunju LP, You L, Zhang Y, Daignault S, Montie JE, Lee CT. Lymphovascular invasion of urothelial cancer in matched transurethral bladder tumor resection and radical cystectomy specimens. J Urol. 2008. 180:1928–1932.16. Lee SE, Jeong IG, Ku JH, Kwak C, Lee E, Jeong JS. Impact of transurethral resection of bladder tumor: analysis of cystectomy specimens to evaluate for residual tumor. Urology. 2004. 63:873–877.17. Cho KS, Seo HK, Joung JY, Park WS, Ro JY, Han KS, et al. Lymphovascular invasion in transurethral resection specimens as predictor of progression and metastasis in patients with newly diagnosed T1 bladder urothelial cancer. J Urol. 2009. 182:2625–2630.18. Chang SS, McKiernan JM, Amin M, Bochner BH, Campbell S, Gospodarowicz MK, et al. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. Urinary bladder. AJCC cancer staging manual. 2010. 7th ed. New York: Springer;497–505.19. Dighe MK, Bhargava P, Wright J. Urinary bladder masses: techniques, imaging spectrum, and staging. J Comput Assist Tomogr. 2011. 35:411–424.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative ventilation and hemodynamic change due to bladder perforation during transurethral resection of a bladder tumor: A case report
- Sudden hypothermia after bladder perforation during transurethral bladder tumor resection: A case report
- Effects of Simultaneous Transurethral Resection of Non-Muscle-Invasive Bladder Cancer and Benign Prostatic Hyperplasia
- Bladder Preservation Management for Muscle Invasive Bladder Cancer
- Recurrence of Subepithelial Non-Muscle Invasive Bladder Cancer Following Transurethral Resection: A Case Report
