Infect Chemother.
2011 Aug;43(4):343-348. 10.3947/ic.2011.43.4.343.
Clinical Characteristics and Outcome of Vascular Access Infections in Hemodialysis Patients
- Affiliations
-
- 1Department of Internal Medicine, Soon Chun Hyang University College of Medicine, Seoul, Korea. mdchoo@schmc.ac.kr
- KMID: 1936071
- DOI: http://doi.org/10.3947/ic.2011.43.4.343
Abstract
- BACKGROUND
Infections are the second leading cause of morbidity and mortality in hemodialysis patients. Vascular access is a major risk factor for infection-related hospitalization and mortality. This study aimed to characterize the presenting features and outcome of vascular access infection in hemodialysis patients.
MATERIALS AND METHODS
Between May 2003 and March 2010, 224 patients admitted to a 750 bed tertiary care hospital for treatment of vascular access infection were retrospectively analyzed. Vascular access infections were defined by local infection signs (pus or redness) at the vascular access site or by a positive blood culture with no known source other than the vascular access.
RESULTS
Of the 224 patients, 179 (79.7%) had an arteriovenous (AV) graft, 28 (12.5%) had a tunneled cuffed catheter, 12 (5.4%) had AV fistulas, and five (2.2%) had a temporary central catheter. The mean+/-SD time between the creation of each type of vascular access and onset of infection were as follows: temporary central catheter 46.6+/-36.9 days, tunneled cuffed catheter 180.3+/-168.8 days, AV fistulas 928.6+/-1,299.7 days, and AV graft 1,066.3+/-1321.1 days (P value=0.006). The most common causative organism was Staphylococcus aureus (62.5%; methicillin-susceptible 35.2%, methicillin-resistant 27.3%) followed by coagulase negative staphylococci (17.0%) and gram negative bacilli (15.9%). The involved vascular accesses in infected cases were: temporary central catheter (4/5, 80%), tunneled cuffed catheter (13/27, 48%), AV graft (68/179, 38%) and AV fistulas (4/12, 33%). The complications of vascular access infection included septic pulmonary embolism (n=9, 4%), pneumonia (n=9, 4%), endocarditis (n=6, 2.7%), osteomyelitis (n=3, 1.3%) and abdominal abscess (n=2, 0.9%). A multivariable analysis showed that Staphylococcus aureus was a risk factor of septic pulmonary embolism and osteomyelitis. The all-cause mortality was 8.4%, 30-day mortality was 2.2% and infection-related mortality was 5.4%.
CONCLUSIONS
Staphylococcus was responsible for 79.5% of infections, with methicillin-susceptible S. aureus being the most commonly implicated strain. Temporary accesses have the potential to become infected earlier. Septic pulmonary embolism and pneumonia were common complications. Efforts should be focused on prevention and early detection of VA infection with pulmonary complications.
Keyword
MeSH Terms
-
Abdominal Abscess
Catheter-Related Infections
Catheters
Coagulase
Endocarditis
Fistula
Hospitalization
Humans
Methicillin Resistance
Osteomyelitis
Pneumonia
Pulmonary Embolism
Renal Dialysis
Retrospective Studies
Risk Factors
Sprains and Strains
Staphylococcus
Staphylococcus aureus
Tertiary Healthcare
Transplants
Coagulase
Figure
-
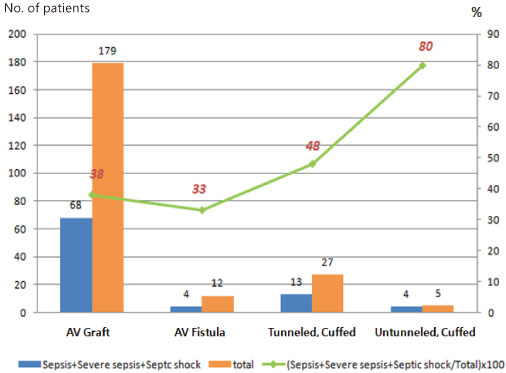
Figure 1 Proportion of sepsis and severe sepsis among those hospitalized with vascular access infection by type of vascular access. AV, arteriovenous; CVC, central venous catheter.
Reference
-
1. ESRD Registry Committee. Korean Society Nephrology. Current renal replacement therapy in Korea: Insan memorial dialysis registry, 2009. Korean J Nephrol. 2010. 29:Suppl 2. S525–S551.2. National Kidney Foundation. Clinical practice guidelines and clinical practice recommendations 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy, vascular access. Am J Kidney Dis. 2006. 48:Suppl 1. S1–S322.3. Vascular Access 2006 Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006. 48:Suppl 1. S176–S247.4. Pearson ML. The Hospital Infection Control Practices Advisory Committee. Guideline for prevention of intravascular device-related infections. Part I. Intravascular device-related infections: an overview. Am J Infect Control. 1996. 24:262–277.
Article5. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992. 101:1644–1655.
Article6. Cook RJ, Ashton RW, Aughenbaugh GL, Ryu JH. Septic pulmonary embolism: presenting features and clinical course of 14 patients. Chest. 2005. 128:162–166.7. Lafrance JP, Rahme E, Lelorier J, Iqbal S. Vascular access-related infections: definitions, incidence rates, and risk factors. Am J Kidney Dis. 2008. 52:982–993.
Article8. Saeed Abdulrahman I, Al-Mueilo SH, Bokhary HA, Ladipo GO, Al-Rubaish A. A prospective study of hemodialysis access-related bacterial infections. J Infect Chemother. 2002. 8:242–246.
Article9. Lee T, Barker J, Allon M. Tunneled catheters in hemodialysis patients: reasons and subsequent outcomes. Am J Kidney Dis. 2005. 46:501–508.
Article10. Qasaimeh GR, El Qaderi S, Al Omari G, Al Badadweh M. Vascular access infection among hemodialysis patients in Northern Jordan: incidence and risk factors. South Med J. 2008. 101:508–512.
Article11. Kessler M, Hoen B, Mayeux D, Hestin D, Fontenaille C. Bacteremia in patients on chronic hemodialysis. A multicenter prospective survey. Nephron. 1993. 64:95–100.12. Minga TE, Flanagan KH, Allon M. Clinical consequences of infected arteriovenous grafts in hemodialysis patients. Am J Kidney Dis. 2001. 38:975–978.
Article13. Lee SJ, Cha SI, Kim CH, Park JY, Jung TH, Jeon KN, Kim GW. Septic pulmonary embolism in Korea: Microbiology, clinicoradiologic features, and treatment outcome. J Infect. 2007. 54:230–234.
Article14. Dhingra RK, Young EW, Hulbert-Shearon TE, Leavey SF, Port FK. Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int. 2001. 60:1443–1451.
Article15. Oliver MJ, Rothwell DM, Fung K, Hux JE, Lok CE. Late creation of vascular access for hemodialysis and increased risk of sepsis. J Am Soc Nephrol. 2004. 15:1936–1942.
Article16. Danese MD, Griffiths RI, Dylan M, Yu HT, Dubois R, Nissenson AR. Mortality differences among organisms causing septicemia in hemodialysis patients. Hemodial Int. 2006. 10:56–62.
Article17. Li Y, Friedman JY, O'Neal BF, Hohenboken MJ, Griffiths RI, Stryjewski ME, Middleton JP, Schulman KA, Inrig JK, Fowler VG Jr, Reed SD. Outcomes of Staphylococcus aureus infection in hemodialysis-dependent patients. Clin J Am Soc Nephrol. 2009. 4:428–434.
Article18. Taylor G, Gravel D, Johnston L, Embil J, Holton D, Paton S. Canadian Hospital Epidemiology Committee. Canadian Nosocomial Infection Surveillance Program. Prospective surveillance for primary bloodstream infections occurring in Canadian hemodialysis units. Infect Control Hosp Epidemiol. 2002. 23:716–720.
Article19. Hoen B, Paul-Dauphin A, Hestin D, Kessler M. EPIBACDIAL: a multicenter prospective study of risk factors for bacteremia in chronic hemodialysis patients. J Am Soc Nephrol. 1998. 9:869–876.
Article20. McCarthy JT, Steckelberg JM. Infective endocarditis in patients receiving long-term hemodialysis. Mayo Clin Proc. 2000. 75:1008–1014.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- History and Development of Vascular Access and Its Impact on Hemodialysis Outcome
- The pathophysiology and inhibition of hemodialysis vascular access stenosis
- Impacts of monthly arteriovenous fistula flow surveillance on hemodialysis access thrombosis and loss
- Clinical Evaluation of Use of Permcath(R) in Patients with Poor Vascular Access
- Analysis of the Outcome of Tunneled Hemodialysis Catheters in Children according to the Indications for Use
