Sarcoidosis Presenting with Massive Pleural Effusion and Elevated Serum and Pleural Fluid Carbohydrate Antigen-125 Levels
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, The Institute of Chest Diseases, Yonsei University College of Medicine, Seoul, Korea. pms70@yuhs.ac
- KMID: 1842925
- DOI: http://doi.org/10.4046/trd.2012.73.6.320
Abstract
- A 55-year-old woman was admitted for an elevated serum carbohydrate antigen-125 (CA-125) level, and a left pleural effusion, which were detected at a routine health examination. Computed tomography of the chest was performed upon admission, revealing extensive bilateral paratracheal and mediastinal lymph node enlargement with a massive left-sided pleural effusion. Subsequent analysis of the pleural fluid demonstrated consistency with an exudate, no evidence of malignant cells, and a normal adenosine deaminase. However, the pleural fluid and serum CA-125 levels were 2,846.8 U/mL and 229.5 U/mL, respectively. A positron emission tomography did not reveal any primary focus of malignancy. Finally, a surgical mediastinoscopic biopsy of several mediastinal lymph nodes was performed, revealing non-necrotizing granulomas, consistent with sarcoidosis. After a month of treatment of prednisolone, the left pleural effusion had resolved, and after 2 months the serum CA-125 level was normalized.
Keyword
MeSH Terms
Figure
-
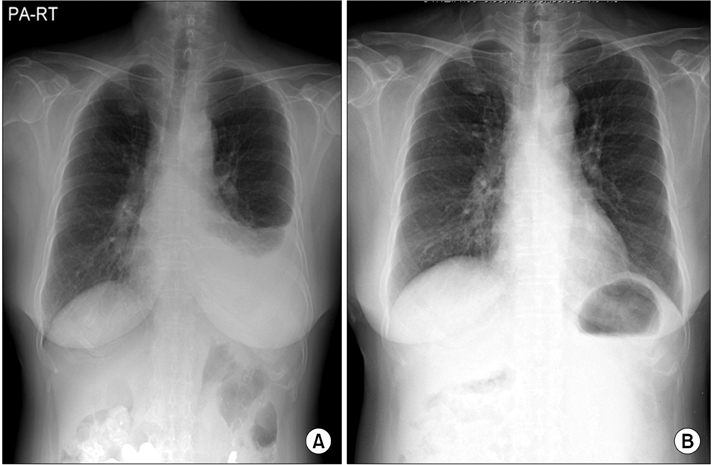
Figure 1 (A) The initial chest X-ray showed a left-sided massive pleural effusion, which disappeared after 2 months of medication with oral prednisolone (B).
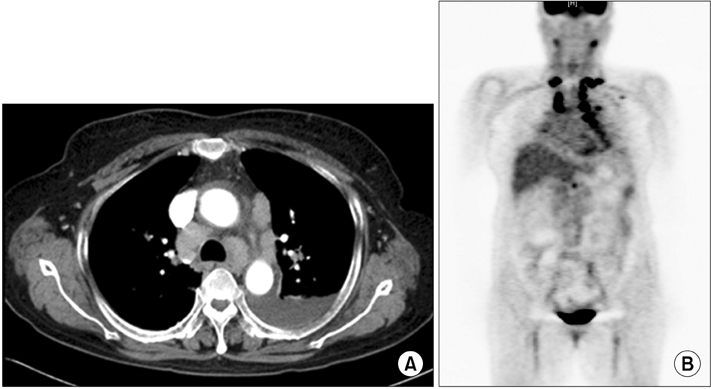
Figure 2 (A) The initial chest computed tomography showed a left-sided pleural effusion and mediastinal lymph nodes enlargement. (B) The 18F-fluorodeoxyglucose-positronemission tomography revealed intense uptake on the bilateral paratracheal, hilar, and supraclavicular lymph nodes.
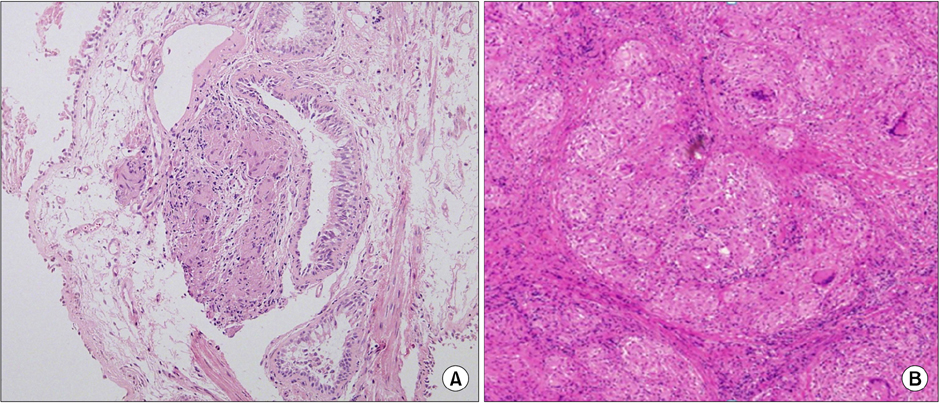
Figure 3 (A) The fiberoptic bronchoscopic biopsy revealed non-necrotizing granulomas in the bronchial wall (H&E stain, ×100). (B) The mediastinoscopic biopsy of right paratracheal lymph node revealed that all normal structures were entirely replaced by non-caseating granulomas, each composed of aggregates of tightly clustered epithelioid cells (H&E stain, ×400).
Reference
-
1. Huggins JT, Doelken P, Sahn SA, King L, Judson MA. Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006. 129:1599–1604.2. Kalluri M, Judson MA. Sarcoidosis associated with an elevated serum CA 125 level: description of a case and a review of the literature. Am J Med Sci. 2007. 334:441–443.3. Salerno D. Sarcoidosis pleural effusion: a not so common feature of a well known pulmonary disease. Respir Care. 2010. 55:478–480.4. Soskel NT, Sharma OP. Pleural involvement in sarcoidosis. Curr Opin Pulm Med. 2000. 6:455–468.5. Durand DV, Dellinger A, Guerin C, Guerin JC, Levrat R. Pleural sarcoidosis: one case presenting with an eosinophilic effusion. Thorax. 1984. 39:468–469.6. Cohen M, Sahn SA. Resolution of pleural effusions. Chest. 2001. 119:1547–1562.7. Mansour M, Linden ER, Colby S, Posner G, Marsh F Jr. Elevation of carcinoembryonic antigen and CA-125 in a patient with multivisceral tuberculosis. J Natl Med Assoc. 1997. 89:142–143.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Meigs' syndrome associated with elevated serum CA 125 level and hemoperitoneum
- Lupus nephritis presenting with massive ascites and pleural effusion (pseudo-pseudo Meigs’ syndrome)
- Postmenopausal Meigs' Syndrome in Elevated CA-125: A Case Report
- Diagnostic Value of LDH and its Isoenzyme in Pleural Effusion
- A Case of Chronic Pancreatitis with Massive Pleural Effusion
