Muscular Sarcoidosis Detected by F-18 FDG PET/CT in a Hypercalcemic Patient
- Affiliations
-
- 1Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. drkhs@catholic.ac.kr
- KMID: 1793060
- DOI: http://doi.org/10.3346/jkms.2013.28.9.1399
Abstract
- Sarcoidosis is a systemic granulomatous disease of unknown etiology that involves many organs, occasionally mimicking malignancy. We herein report a 50-yr-old woman of muscular sarcoidosis of chronic myopathic type, manifested by hypercalcemia and muscle wasting. Besides insignificant hilar lymphadenopathy, her sarcoidosis was confined to generalized atrophic muscles and therefore, F-18 FDG PET/CT alone among conventional imaging studies provided diagnostic clues for the non-parathyroid-related hypercalcemia. On follow-up PET/CT during low-dose steroid treatment, FDG uptake in the muscles disappeared whereas that in the hilar lymph nodes remained. PET/CT may be useful in the evaluation of unexpected disease extent and monitoring treatment response in suspected or known sarcoidosis patients.
Keyword
MeSH Terms
-
Female
Fluorodeoxyglucose F18/*diagnostic use
Humans
Hypercalcemia/complications/*diagnosis
Kidney Calculi/complications/diagnosis
Lymph Nodes/radionuclide imaging
Middle Aged
Positron-Emission Tomography
Radiopharmaceuticals/*diagnostic use
Sarcoidosis/complications/drug therapy/*radionuclide imaging
Steroids/therapeutic use
Tomography, X-Ray Computed
Fluorodeoxyglucose F18
Radiopharmaceuticals
Steroids
Figure
-
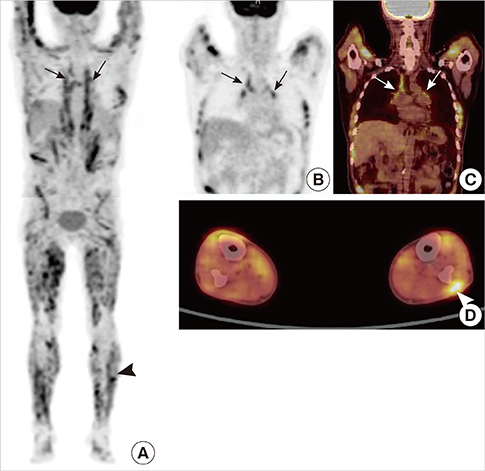
Fig. 1 F-18 FDG PET/CT findings. In maximum intensity projection (MIP) (A) and coronal (B, C) images of PET/CT, increased uptake was noted in mediastinal and bilateral hilar lymph nodes (arrows). In addition, multiple streaky and dotted muscular uptakes were noted along whole body. Nodular uptake was seen in left lower lateral leg (arrowhead) in MIP (A) and transaxial (D) images, and excisional biopsy was performed in this mass.

Fig. 2 Histologic result. Biopsy specimen was obtained from muscular mass of left lower leg. Microscopic findings (hematoxylin-eosin stain) demonstrated non-necrotizing granulomas (arrows) with multinucleated giant cell (arrowhead) and without acid-fast bacilli or fungi. The histology was consistent with muscular sarcoidosis.

Fig. 3 Follow-up PET/CT finding. In MIP image, previously noted multiple muscular uptakes were no longer seen. However, increased uptake in mediastinal and bilateral hilar lymph nodes persisted (arrows).
Reference
-
1. Vardhanabhuti V, Venkatanarasimha N, Bhatnagar G, Maviki M, Iyengar S, Adams WM, Suresh P. Extra-pulmonary manifestations of sarcoidosis. Clin Radiol. 2012; 67:263–276.2. Spagnolo P, Luppi F, Roversi P, Cerri S, Fabbri LM, Richeldi L. Sarcoidosis: challenging diagnostic aspects of an old disease. Am J Med. 2012; 125:118–125.3. Silverstein A, Siltzbach LE. Muscle involvement in sarcoidosis: asymptomatic, myositis, and myopathy. Arch Neurol. 1969; 21:235–241.4. Marie I, Lahaxe L, Vera P, Edet-Samson A. Follow-up of muscular sarcoidosis using fluorodeoxyglucose positron emission tomography. QJM. 2010; 103:1000–1002.5. Tohme-Noun C, Le Breton C, Sobotka A, Boumenir ZE, Milleron B, Carette MF, Khalil A. Imaging findings in three cases of the nodular type of muscular sarcoidosis. AJR Am J Roentgenol. 2004; 183:995–999.6. Costabel U. Skeletal muscle weakness, fatigue and sarcoidosis. Thorax. 2005; 60:1–2.7. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med. 1997; 336:1224–1234.8. Conron M, Young C, Beynon HL. Calcium metabolism in sarcoidosis and its clinical implications. Rheumatology (Oxford). 2000; 39:707–713.9. Richmond BW, Drake WP. Vitamin D, innate immunity, and sarcoidosis granulomatous inflammation: insights from mycobacterial research. Curr Opin Pulm Med. 2010; 16:461–464.10. Baughman RP, Lower EE, du Bois RM. Sarcoidosis. Lancet. 2003; 361:1111–1118.11. Studdy PR, Lapworth R, Bird R. Angiotensin-converting enzyme and its clinical significance: a review. J Clin Pathol. 1983; 36:938–947.12. Meller J, Sahlmann CO, Scheel AK. 18F-FDG PET and PET/CT in fever of unknown origin. J Nucl Med. 2007; 48:35–45.13. Solav SV. FDG PET/CT in evaluation of pyrexia of unknown origin. Clin Nucl Med. 2011; 36:e81–e86.14. Cecchin D, Motta R, Zucchetta P, Bui F, Basso SM, Lumachi F. Imaging studies in hypercalcemia. Curr Med Chem. 2011; 18:3485–3493.15. Culverwell AD, Scarsbrook AF, Chowdhury FU. False-positive uptake on 2-[18F]-fluoro-2-deoxy-D-glucose (FDG) positron-emission tomography/computed tomography (PET/CT) in oncological imaging. Clin Radiol. 2011; 66:366–382.16. Braun JJ, Kessler R, Constantinesco A, Imperiale A. 18F-FDG PET/CT in sarcoidosis management: review and report of 20 cases. Eur J Nucl Med Mol Imaging. 2008; 35:1537–1543.17. Aide N, Benayoun M, Kerrou K, Khalil A, Cadranel J, Talbot JN. Impact of [18F]-fluorodeoxyglucose ([18F]-FDG) imaging in sarcoidosis: unsuspected neurosarcoidosis discovered by [18F]-FDG PET and early metabolic response to corticosteroid therapy. Br J Radiol. 2007; 80:e67–e71.18. Nishiyama Y, Yamamoto Y, Fukunaga K, Takinami H, Iwado Y, Satoh K, Ohkawa M. Comparative evaluation of 18F-FDG PET and 67Ga scintigraphy in patients with sarcoidosis. J Nucl Med. 2006; 47:1571–1576.19. Sohn HS, Kim EN. A case of muscular sarcoidosis diagnosed by gallium-67 scintigraphy and magnetic resonance imaging. Korean J Nucl Med. 1999; 33:543–548.20. Lee JH, Lim YJ, Lee S, Joo KB, Choi YY, Park CK, Lee YH. Early-onset childhood sarcoidosis with incidental multiple enchondromatosis. J Korean Med Sci. 2012; 27:96–100.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Incidentally Detected Nasopharyngeal Tuberculosis on F-18 FDG PET/CT
- The Role of Multimodality Imaging in Cardiac Sarcoidosis
- Growing Cardiac Hemangioma on Serial F-18 FDG PET/CT
- F-18 FDG PET/CT Finding in Solid Pseudo-papillary Tumor of the Pancreas 6 years After Initial Diagnosis
- Multiple Skeletal Muscle Metastases in a Case of Transitional Cell Carcinoma of Bladder Detected by F-18 FDG PET/CT
