J Korean Med Sci.
2011 Oct;26(10):1322-1327. 10.3346/jkms.2011.26.10.1322.
High-sensitivity C-reactive Protein Can Predict Major Adverse Cardiovascular Events in Korean Patients with Type 2 Diabetes
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Kwandong University, Goyang, Korea.
- 2Department of Endocrinology, College of Medicine, Kwandong University, Goyang, Korea. khj1212@kwandong.ac.kr
- KMID: 1785990
- DOI: http://doi.org/10.3346/jkms.2011.26.10.1322
Abstract
- Inflammation is thought to play a role in the pathogenesis of major adverse cardiovascular events (MACE). It has been suggested that the measurement of markers of inflammation may aid in predicting the risk of such events. Here, the relationship between high-sensitivity C-reactive protein (hs-CRP) levels and MACE in Korean patients with type 2 diabetes is assessed. A retrospective cohort study was conducted as a follow-up among 1,558 patients with type 2 diabetes and without cardiovascular diseases over a mean period of 55.5 months. A Cox proportional-hazards model was used to determine whether increased hs-CRP levels are useful as a predictor for future MACE. The hazard ratio of MACE was 1.77 (95% CI; 1.16-2.71) in subjects who had the highest hs-CRP levels (> 0.21 mg/dL) compared to subjects who had the lowest hs-CRP levels (< 0.08 mg/dL), after adjusting for age, regular physical activity, current smoking, and duration of diabetes. The present results indicate that high hs-CRP levels can act as a predictor for the MACE occurrence in Korean patients with type 2 diabetes.
MeSH Terms
-
Adult
Aged
Biological Markers/*blood
C-Reactive Protein/*analysis
Cardiovascular Diseases/blood/*epidemiology/etiology
Cohort Studies
Diabetes Mellitus, Type 2/blood/*complications/epidemiology
Female
Follow-Up Studies
Humans
Inflammation
Male
Middle Aged
Predictive Value of Tests
Prognosis
Proportional Hazards Models
Republic of Korea
Retrospective Studies
Sensitivity and Specificity
Figure
-
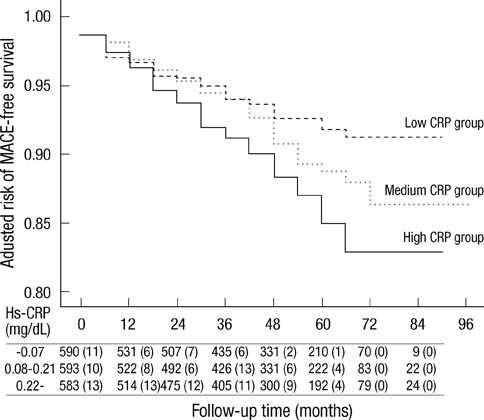
Fig. 1 Association between baseline C-reactive protein tertile and a risk for a Major adverse cardiovascular event (MACE). Risk estimates were calculated using a multivariable Cox regression model, adjusting for age, sex, duration of DM, current smoking physical acitivity, and total cholesterol P value is <0.009 between low-level hs-CRP and high-level hs-CRP group.
Reference
-
1. Hartge MM, Unger T, Kintscher U. The endothelium and vascular inflammation in diabetes. Diab Vasc Dis Res. 2007. 4:84–88.2. Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith SC Jr, Sowers JR. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999. 100:1134–1146.3. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000. 342:836–843.4. Rost NS, Wolf PA, Kase CS, Kelly-Hayes M, Silbershatz H, Massaro JM, D'Agostino RB, Franzblau C, Wilson PW. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: the Framingham Study. Stroke. 2001. 32:2575–2579.5. Ridker PM, Rifai N, Rose N, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular event. N Engl J Med. 2002. 347:1557–1565.6. Ridker PM, Stampfer MJ, Rifai N. Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA. 2001. 285:2481–2485.7. Kang ES, Kim HJ, Ahn CW, Park CW, Cha BS, Lim SK, Kim KR, Lee HC. Relationship of serum high sensitivity C-reactive protein to metabolic syndrome and microvascular complications in type 2 diabetes. Diabetes Res Clin Pract. 2005. 69:151–159.8. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972. 18:499–502.9. Ryan TJ, Antman EM, Brooks NH, Califf RM, Hillis LD, Hiratzka LF, Rapaport E, Riegel B, Russell RO, Smith EE 3rd, Weaver WD, Gibbons RJ, Alpert JS, Eagle KA, Gardner TJ, Garson A Jr, Gregoratos G, Smith SC Jr. 1999 update: ACC/AHA Guidelines for the Management of Patients with Acute Myocardial Infarction: Executive Summary and Recommendations: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). Circulation. 1999. 100:1016–1030.10. WHO MONICA Project Principal Investigators. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J Clin Epidemiol. 1988. 41:105–114.11. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC Jr, Stone NJ. Coordinating Committee of the National Cholesterol Education Program. Implications of recent clinical trials for the National Cholesterol Education Program adult treatment panel III guidelines. J Am Coll Cardiol. 2004. 44:720–732.12. Bierman EL. Atherogenesis in diabetes. Arterioscler Thromb. 1992. 12:647–656.13. Wägner AM, Pérez A, Calvo F, Bonet R, Castellví A, Ordõñez J. Apolipoprotein(B) identifies dyslipidemic phenotypes associated with cardiovascular risk in normocholesterolemic type 2 diabetic patients. Diabetes Care. 1999. 22:812–817.14. Laakso M, Lehto S, Penttilä I, Pyörälä K. Lipids and lipoproteins predicting coronary heart disease mortality and morbidity in patients with non-insulin-dependent diabetes. Circulation. 1993. 88:1421–1430.15. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ. 1998. 317:703–713.16. Wen J, Liang Y, Wang F, Sun L, Guo Y, Duan X, Liu X, Wong TY, Lu X, Wang N. C-reactive protein, gamma-glutamyltransferase and type 2 diabetes in a Chinese population. Clin Chim Acta. 2010. 411:198–203.17. Sitzer M, Markus HS, Mendall MA, Liehr R, Knorr U, Steinmetz H. C-reactive protein and carotid intimal medial thickness in a community population. J Cardiovasc Risk. 2002. 9:97–103.18. Hashimoto H, Kitagawa K, Hougaku H, Shimizu Y, Sakaguchi M, Nagai Y, Iyama S, Yamanishi H, Matsumoto M, Hori M. C-reactive protein in an independent predictor of the rate of increase in early carotid atherosclerosis. Circulation. 2001. 104:63–67.19. Kang ES, Kim HJ, Ahn CW, Park CW, Cha BS, Lim SK, Kim KR, Lee HC. Relationship of serum high sensitivity C-reactive protein to metabolic syndrome and microvascular complications in type 2 diabetes. Diabetes Res Clin Pract. 2005. 69:151–159.20. Palmieri V, Tracy RP, Roman MJ, Liu JE, Best LG, Bella JN, Robbins DC, Howard BV, Devereux RB. Strong Heart Study. Relation of left ventricular hypertrophy to inflammation and albuminuria in adults with type 2 diabetes: the strong heart study. Diabetes Care. 2003. 26:2764–2769.21. Matsumoto K, Sera Y, Abe Y, Ueki Y, Tominaga T, Miyake S. Inflammation and insulin resistance are independently related to all-cause of death and cardiovascular events in Japanese patients with type 2 diabetes mellitus. Atherosclerosis. 2003. 169:317–321.22. Bruno G, Fornengo P, Novelli G, Panero F, Perotto M, Segre O, Zucco C, Deambrogio P, Bargero G, Perin PC. C-reactive protein and 5-year survival in type 2 diabetes: the Casale Monferrato Study. Diabetes. 2009. 58:926–933.23. Piéroni L, Bastard JP, Piton A, Khalil L, Hainque B, Jardel C. Interpretation of circulating C-reactive protein levels in adults: body mass index and gender are a must. Diabetes Metab. 2003. 29:133–138.24. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC Jr, Taubert K, Tracy RP, Vinicor F. Centers for Disease Control and Prevention. American Heart Association. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003. 107:499–511.25. Soinio M, Marniemi J, Laakso M, Lehto S, Rönnemaa T. High-sensitivity C-reactive protein and coronary heart disease mortality in patients with type 2 diabetes: a 7-year follow-up study. Diabetes Care. 2006. 29:329–333.26. Schulze MB, Rimm EB, Li T, Rifai N, Stampfer MJ, Hu FB. C-reactive protein and incident cardiovascular events among men with diabetes. Diabetes Care. 2004. 27:889–894.27. Noh HJ, Kwon NH, Joo SB. Severity of coronary atherosclerosis: influence of metabolic syndrome risk factor clustering and hs-CRP. Korean Circ J. 2006. 36:802–808.28. Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, Tsai J, Orazem J, Magorien RD, O'Shaughnessy C, Ganz P. Reversal of Atherosclerosis with Aggressive Lipid Lowering (REVERSAL) Investigators. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med. 2005. 352:29–38.29. Ridker PM, Cannon CP, Morrow D, Rifai N, Rose LM, McCabe CH, Pfeffer MA, Braunwald E. Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22) Investigators. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005. 352:20–28.30. Jo HJ, Park MJ, Cha JK. The changes of high sensitive C-reactive protein by atorvastatin 20 mg in acute ischemic stroke. J Korean Neurol Assoc. 2007. 25:70–74.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Role and Clinical Significance of High-Sensitivity C-Reactive Protein in Cardiovascular Disease
- The Triglyceride-Glucose Index Can Predict Long-Term Major Adverse Cardiovascular Events in Turkish Patients With High Cardiovascular Risk
- Prevalent Rate of Nonalbuminuric Renal Insufficiency and Its Association with Cardiovascular Disease Event in Korean Type 2 Diabetes
- Paradigm Shift for the Treatment of Type 2 Diabetes Mellitus in Patients with Cardiovascular Disease: Cardiologist's Perspective
- Association between Dietary Protein Intake and Serum High-Sensitivity C-Reactive Protein Level in the Korean Elderly with Diabetes: Based on the Korea National Health and Nutrition Examination Survey 2016–2018
