Yonsei Med J.
2012 Jan;53(1):76-82. 10.3349/ymj.2012.53.1.76.
The Effects of a Bidirectional Cavo-Tricuspid Isthmus Block in Persistent Atrial Fibrillation
- Affiliations
-
- 1Cardiology Division, Department of Internal Medicine, Kyung Hee University College of Medicine, Seoul, Korea.
- 2Cardiology Division, Kang-Nam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
- 3Cardiology Division, Yonsei Cardiovascular Center and Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul, Korea. mhlee@yuhs.ac
- KMID: 1779689
- DOI: http://doi.org/10.3349/ymj.2012.53.1.76
Abstract
- PURPOSE
Hybrid therapy with catheter ablation of the cavo-tricuspid isthmus (CTI) and continuation of anti-arrhythmic drugs (AAD), or electrical cardioversion with AADs might be alternative treatments for patients with persistent atrial fibrillation (AF). The goal of study was to assess the long term success rate of hybrid therapy for persistent AF compared to antiarrhythmic medication therapy after electrical cardioversion and identify the independent risk factors associated with recurrence after hybrid therapy.
MATERIALS AND METHODS
A total of 32 patients with persistent AF who developed atrial flutter after the administration of a class Ic or III anti-arrhythmic drug were enrolled. This group was compared with a group (33 patients) who underwent cardioversion and received direct current cardioversion with AADs. Baseline data were collected, and electrocardiogram and symptom driven Holter monitoring were performed every 2-4 months.
RESULTS
There was no significant difference in the baseline characteristics between the groups. The 12 month atrial arrhythmia free survival was better in the hybrid group, 49.0% vs. 33.1%, p=0.048. However, during a mean 55.7+/-43.0 months of follow up, the improved survival rate regressed (p=0.25). A larger left atrium size was an independent risk factor for the recurrence of AF after adjusting for confounding factors.
CONCLUSION
Despite favorable outcome during 12 month, the CTI block with AADs showed outcomes similar to AAD therapy after electrical cardioversion over a 12 month follow up period. Minimal substrate modification with AADs might be an alternative treatment for persistent AF with minimal atrial remodeling.
MeSH Terms
-
Adult
Aged
Anti-Arrhythmia Agents/*therapeutic use
Atrial Fibrillation/*drug therapy/mortality/*surgery
Catheter Ablation/*methods/mortality
Combined Modality Therapy
*Electric Countershock/mortality
Female
Humans
Male
Middle Aged
Postoperative Complications/mortality/prevention & control
Retrospective Studies
Risk Factors
*Tricuspid Valve
Figure
-

Fig. 1 Comparision of 12 month event free survival curves between hybrid and electrical cardioversion group patients. AF, atrial fibrillation.
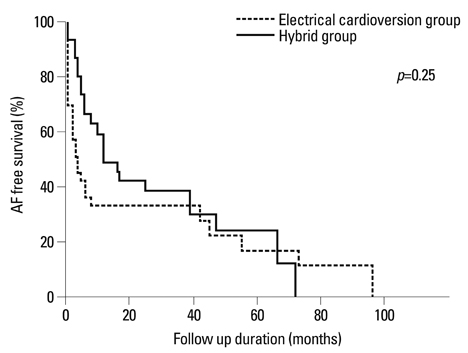
Fig. 2 Comparision of long term event free survival curves between hybrid and electrical cardioversion group patients. AF, atrial fibrillation.
Reference
-
1. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011. 123:e269–e367.2. Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi F Jr, et al. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med. 2006. 354:934–941.
Article3. Knecht S, Hocini M, Wright M, Lellouche N, O'Neill MD, Matsuo S, et al. Left atrial linear lesions are required for successful treatment of persistent atrial fibrillation. Eur Heart J. 2008. 29:2359–2366.
Article4. Stabile G, Bertaglia E, Turco P, Zoppo F, Iuliano A, Zerbo F, et al. Role of pulmonary veins isolation in persistent atrial fibrillation ablation: the pulmonary vein isolation in persistent atrial fibrillation (PIPA) study. Pacing Clin Electrophysiol. 2009. 32:Suppl 1. S116–S119.5. Huang DT, Monahan KM, Zimetbaum P, Papageorgiou P, Epstein LM, Josephson ME. Hybrid pharmacologic and ablative therapy: a novel and effective approach for the management of atrial fibrillation. J Cardiovasc Electrophysiol. 1998. 9:462–469.
Article6. Schumacher B, Jung W, Lewalter T, Vahlhaus C, Wolpert C, Lüderitz B. Radiofrequency ablation of atrial flutter due to administration of class IC antiarrhythmic drugs for atrial fibrillation. Am J Cardiol. 1999. 83:710–713.
Article7. Reithmann C, Hoffmann E, Spitzlberger G, Dorwarth U, Gerth A, Remp T, et al. Catheter ablation of atrial flutter due to amiodarone therapy for paroxysmal atrial fibrillation. Eur Heart J. 2000. 21:565–572.
Article8. Turco P, De Simone A, La Rocca V, El Jamal B, Nocerino P, Astarita C, et al. Long-term results of hybrid therapy in patients with atrial fibrillation who develop atrial flutter during flecainide infusion. Pacing Clin Electrophysiol. 2005. 28:Suppl 1. S124–S127.
Article9. Stevenson WG, Sager PT, Friedman PL. Entrainment techniques for mapping atrial and ventricular tachycardias. J Cardiovasc Electrophysiol. 1995. 6:201–216.
Article10. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998. 339:659–666.
Article11. Lazar S, Dixit S, Marchlinski FE, Callans DJ, Gerstenfeld EP. Presence of left-to-right atrial frequency gradient in paroxysmal but not persistent atrial fibrillation in humans. Circulation. 2004. 110:3181–3186.
Article12. Murdock CJ, Kyles AE, Yeung-Lai-Wah JA, Qi A, Vorderbrugge S, Kerr CR. Atrial flutter in patients treated for atrial fibrillation with propafenone. Am J Cardiol. 1990. 66:755–757.
Article13. Tai CT, Chiang CE, Lee SH, Chen YJ, Yu WC, Feng AN, et al. Persistent atrial flutter in patients treated for atrial fibrillation with amiodarone and propafenone: electrophysiologic characteristics, radiofrequency catheter ablation, and risk prediction. J Cardiovasc Electrophysiol. 1999. 10:1180–1187.
Article14. Nabar A, Rodriguez LM, Timmermans C, Smeets JL, Wellens HJ. Radiofrequency ablation of "class IC atrial flutter" in patients with resistant atrial fibrillation. Am J Cardiol. 1999. 83:785–787.
Article15. Nabar A, Rodriguez LM, Timmermans C, van Mechelen R, Wellens HJ. Class IC antiarrhythmic drug induced atrial flutter: electrocardiographic and electrophysiological findings and their importance for long term outcome after right atrial isthmus ablation. Heart. 2001. 85:424–429.
Article16. Brooks AG, Stiles MK, Laborderie J, Lau DH, Kuklik P, Shipp NJ, et al. Outcomes of long-standing persistent atrial fibrillation ablation: a systematic review. Heart Rhythm. 2010. 7:835–846.
Article17. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, et al. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005. 111:1100–1105.
Article18. Fetsch T, Bauer P, Engberding R, Koch HP, Lukl J, Meinertz T, et al. Prevention of atrial fibrillation after cardioversion: results of the PAFAC trial. Eur Heart J. 2004. 25:1385–1394.
Article19. Reithmann C, Dorwarth U, Dugas M, Hahnefeld A, Ramamurthy S, Remp T, et al. Risk factors for recurrence of atrial fibrillation in patients undergoing hybrid therapy for antiarrhythmic drug-induced atrial flutter. Eur Heart J. 2003. 24:1264–1272.
Article20. Stabile G, De Simone A, Turco P, La Rocca V, Nocerino P, Astarita C, et al. Response to flecainide infusion predicts long-term success of hybrid pharmacologic and ablation therapy in patients with atrial fibrillation. J Am Coll Cardiol. 2001. 37:1639–1644.
Article21. Wazni O, Marrouche NF, Martin DO, Gillinov AM, Saliba W, Saad E, et al. Randomized study comparing combined pulmonary vein-left atrial junction disconnection and cavotricuspid isthmus ablation versus pulmonary vein-left atrial junction disconnection alone in patients presenting with typical atrial flutter and atrial fibrillation. Circulation. 2003. 108:2479–2483.
Article22. Ortiz J, Niwano S, Abe H, Rudy Y, Johnson NJ, Waldo AL. Mapping the conversion of atrial flutter to atrial fibrillation and atrial fibrillation to atrial flutter. Insights into mechanisms. Circ Res. 1994. 74:882–894.
Article23. Waldo AL, Feld GK. Inter-relationships of atrial fibrillation and atrial flutter mechanisms and clinical implications. J Am Coll Cardiol. 2008. 51:779–786.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bidirectional Cavopulmonary Shunt for Isolated Right Ventricular Endomyocardial Fibrosis
- Ethanol Infusion in the Vein of Marshall in a Patient with Persistent Atrial Fibrillation
- Tricuspid atresia associated with double orifice mitral valve and coronary sinus septal defect
- A Totally Thoracoscopic Ablation for Persistent Atrial Fibrillation
- Persistent Atrial Fibrillation Related to a Congenital Pericardial Defect and Left Atrial Appendage Herniation
