Bupivacaine Induced Cardiac Toxicity Mimicking an Acute Non-ST Segment Elevation Myocardial Infarction
- Affiliations
-
- 1Division of Cardiology, Yonsei University Wonju College of Medicine, Wonju, Korea. carshlee@yonsei.ac.kr
- 2Department of Anesthesiology and Pain Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 1779541
- DOI: http://doi.org/10.3349/ymj.2007.48.2.331
Abstract
- Bupivacaine is widely used as a local anesthetic. Central nervous system (CNS) and cardiovascular toxicity are well known side effects. However, there has been no report of bupivacaine-induced myocardial injury. We present a case of bupivacaine cardiac toxicity mimicking an acute non-ST segment elevation myocardial infarction, which was eventually diagnosed as bupivacaine-induced cardiac toxicity without CNS toxicity. As soon as a healthy young woman at a private clinic was given a spinal anesthesia of 6mg bupivacaine for hemorrhoidectomy, she developed arrhythmia and hypotension. She was transferred to our emergency room. There was an accelerated idioventricular rhythm with ST segment depression on electrocardiogram, coarse breathing sounds with rales on whole lung field and a butterfly sign on the chest radiograph. 2D transthoracic echocardiography (TTE) revealed reduced left ventricle systolic ejection fraction (approximately 27%). There was regional wall motion abnormality of the left ventricle on 2D TTE and the cardiac marker was increased. We diagnosed the patient as having acute non-ST segment elevation myocardial infarction but her impaired cardiac function improved gradually. On the seventh day from admission, there was a complete spontaneous recovery of cardiac function, and coronary angiography revealed a normal coronary artery. Therefore, we firmly believe that bupivacaine directly injures the cardiac cell.
Keyword
MeSH Terms
Figure
-
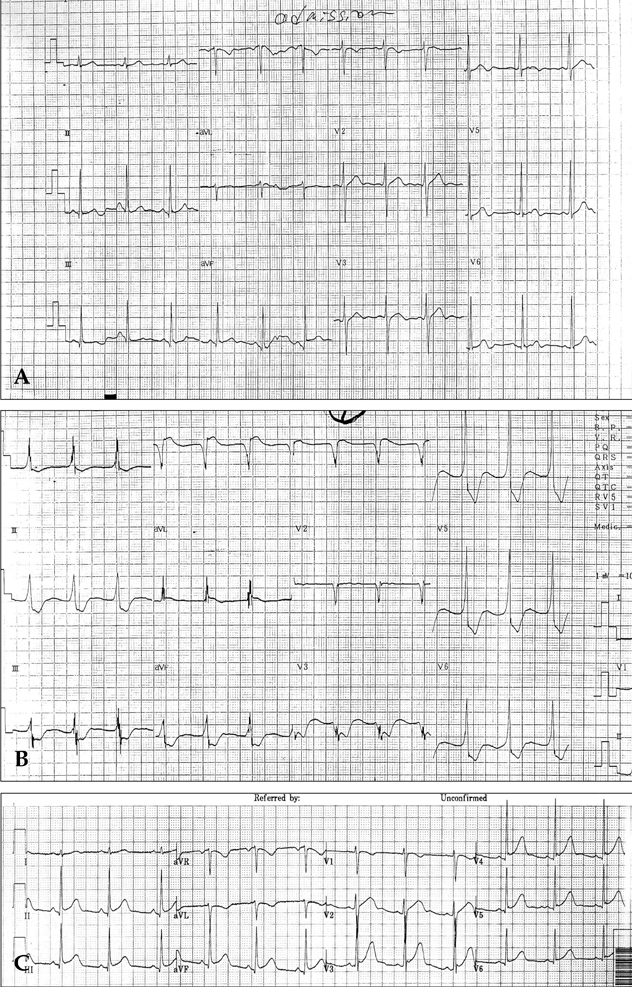
Fig. 1 (A) Patient's electrocardiogram before surgery. (B) Patient's electrocardiogram when she complained of chest discomfort, dyspnea and dizziness after spinal anesthesia. (C) Patient's electrocardiogram on discharge.

Fig. 2 Patient's chest radiographs on arrival (A) at emergency room and on discharge (B).

Fig. 3 (A) 2D TTE findings on arrival at ER. 2D Transthoracic echocardiogram (TTE) showed reduced myocardial contractility, diffuse hypokinesia of the left ventricle, especially akinesia of the anteroseptum of the mid-left ventricle and all segments of the left ventricle at the base, mitral regurgitation of grade I/IV and a reduced left ventricular systolic function (ejection fraction: 27%). (B) 2D TTE findings, 3 days after first examination. 2D TTE revealed a normal sized cardiac chamber with improved left ventricle systolic function (ejection fraction: 51%). (C) 2D TTE findings on discharge. Improved heart function (left ventricle ejection fraction: 71%) and morphologically normal heart.
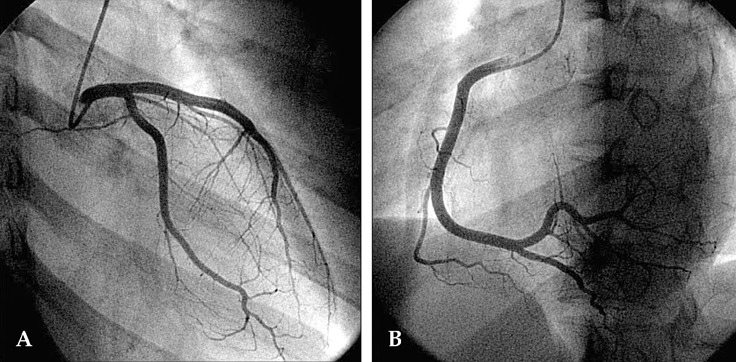
Fig. 4 Coronary angiography. Left (A. normal) and right (B. normal) coronary arteries.
Reference
-
1. Knudsen K, Beckman Suurkula K, Blomberg S, Sjovall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997. 78:507–514.2. Arlock P. Actions of three local anaesthetics: lidocaine, bupivacaine and ropivacaine on guinea pig papillary muscle sodium channels (Vmax). Pharmacol Toxicol. 1988. 63:96–104.3. Clarkson CW, Hondeghem LM. Mechanism for bupivacaine depression of cardiac conduction: fast block of sodium channels during the action potential with slow recovery from block during diastole. Anesthesiology. 1985. 62:396–405.4. Heavner JE. Cardiac toxicity of local anesthetics in the intact isolated heart model: a review. Reg Anesth Pain Med. 2002. 27:545–555.5. Matsouka H, Hamada M, Honda T, Kawakami H, Abe M, Shigematsu Y, et al. Evaluation of acute myocarditis and pericarditis by Gd-DTPA enhanced magnetic resonance imaging. Eur Heart J. 1994. 15:283–284.6. Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005. 352:539–548.7. Moller R, Covino BG. Cardiac electrophysiologic properties of bupivacaine and lidocaine compared with those of ropivacaine, a new amide local anesthetic. Anesthesiology. 1990. 72:322–329.8. Feldman HS, Arthur GR, Pitkanen M, Hurley R, Doucette AM, Covino BG. Treatment of acute systemic toxicity after the rapid intravenous injection of ropivacaine and bupivacaine in the conscious dog. Anesth Analg. 1991. 73:373–384.9. Scott DB, Lee A, Fagan D, Bowler GM, Bloomfield P, Lundh R. Acute toxicity of ropivacaine compared with that of bupivacaine. Anesth Analg. 1989. 69:563–569.10. Coven G, Arpesella R, Ciceri M, Preseglio I, Cardani A. Accelerated idioventricular rhythm during spinal anesthesia for cesarean section. Int J Obstet Anesth. 2003. 12:121–125.
Article11. Cotileas P, Myrianthefs P, Haralambakis A, Cotsopoulos P, Stamatopoulou C, Ladakis C, et al. Bupivacaine-induced myocardial depression and pulmonary edema: a case report. J Electrocardiol. 2000. 33:291–296.
Article12. Sztark F, Malgat M, Dabadie P, Mazat JP. Comparison of the effects of bupivacaine and ropivacaine on heart cell mitochondrial bioenergetics. Anesthesiology. 1998. 88:1340–1349.
Article13. Tanz RD, Heskett T, Loehning RW, Fairfax CA. Comparative cardiotoxicity of bupivacaine and lidocaine in the isolated perfused mammalian heart. Anesth Analg. 1984. 63:549–556.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute ST-Segment Elevation Myocardial Infarction Mimicking Stress Induced Cardiomyopathy; Demonstration of Typical Echocardiographic Finding Correlated with Unusual Distribution of Left Anterior Descending Coronary Artery
- A Case of Acute Myopericarditis with Localized ST Elevation Mimicking Myocardial Infarction
- A Case of ST-Segment Elevation Myocardial Infarction Mimicking Stress-Induced Cardiomyopathy
- A Case of Cardiac Metastasis from Lung Cancer Presented with Persistent ST Segment Elevation Simulating Acute Myocardial Infarction
- ST segment
