A Case of Acute ST-Segment Elevation Myocardial Infarction Mimicking Stress Induced Cardiomyopathy; Demonstration of Typical Echocardiographic Finding Correlated with Unusual Distribution of Left Anterior Descending Coronary Artery
- Affiliations
-
- 1Cardiology Division of Internal Medicine, Cardiocerebrovascular Center, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea. jaehpark@cnuh.co.kr
- KMID: 2177308
- DOI: http://doi.org/10.4250/jcu.2010.18.3.101
Abstract
- Stress-induced cardiomyopathy (SCMP) is diagnosed in 1-2% of patients presenting with symptoms suggestive of acute coronary syndrome. Because of sharing many common clinical features with SCMP, acute ST-segment elevation myocardial infarction (STEMI) can be misdiagnosed as SCMP. However, it can be associated with fatal outcome of the patient. Also, diagnosis of SCMP seems to be always challenging to clinicians, especially in the decision of taking coronary angiography which is still invasive and even risky. Here, we present a case with acute STEMI mimicking SCMP as a result of anatomical variation of coronary circulation. In this patient, prompt and early coronary angiography and stent implantation was very helpful.
Keyword
MeSH Terms
Figure
-
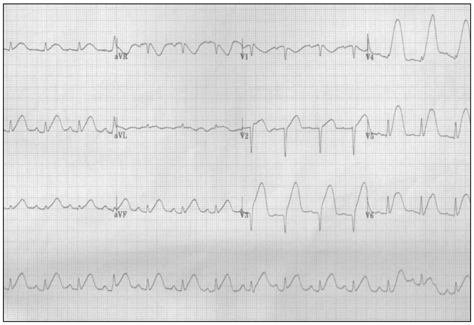
Fig. 1 The initial electrocardiogram shows ST-segment elevation in nearly all leads.
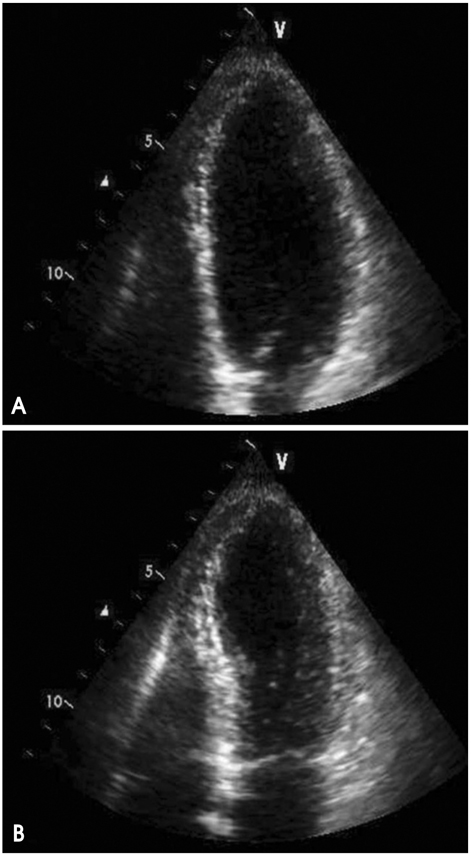
Fig. 2 The echocardiography taken at admission reveals dilated left ventricular apex compatible with typical apical ballooning syndrome (A: end-diastole, and B: end-systole).

Fig. 3 The initial left coronary angiogram demonstrates totally occluded mid portion of the left anterior descending coronary artery (arrow) (A). After successful reperfusion therapy, her left anterior descending coronary artery runs along the apex and supplies to the mid posterior aspect of the left ventricle (B).
Cited by 1 articles
-
Stress Cardiomyopathy Complicated by Left Ventricular Thrombi and Cerebral Infarctions in a Patient with Essential Thrombocythemia
Seung Hwan Hwang, Kye Hun Kim, Hyun Ju Yoon, Young Joon Hong, Ju Han Kim, Young Keun Ahn, Myung Ho Jeong, Jeong Gwan Cho, Jong Chun Park, Jung Chaee Kang
J Cardiovasc Ultrasound. 2011;19(2):87-90. doi: 10.4250/jcu.2011.19.2.87.
Reference
-
1. Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. [Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases]. J Cardiol. 1991. 21:203–214.2. Kurt IH. Coronary artery disease mimicking Tako-tsubo cardiomyopathy: a case report. Cases J. 2009. 2:6374.
Article3. Park JH, Kang SJ, Song JK, Kim HK, Lim CM, Kang DH, Koh Y. Left ventricular apical ballooning due to severe physical stress in patients admitted to the medical ICU. Chest. 2005. 128:296–302.
Article4. Kim EM, Park JH, Park YS, Lee JH, Choi SW, Jeong JO, Seong IW. Catecholamines may play an important role in the pathogenesis of transient mid- and basal ventricular ballooning syndrome. J Korean Med Sci. 2008. 23:898–902.
Article5. Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010. 55:333–341.
Article6. Vidi V, Rajesh V, Singh PP, Mukherjee JT, Lago RM, Venesy DM, Waxman S, Pyne CT, Piemonte TC, Gossman DE, Nesto RW. Clinical characteristics of tako-tsubo cardiomyopathy. Am J Cardiol. 2009. 104:578–582.
Article7. Kawai S, Kitabatake A, Tomoike H. Takotsubo Cardiomyopathy Group. Guidelines for diagnosis of takotsubo (ampulla) cardiomyopathy. Circ J. 2007. 71:990–992.
Article8. Kurisu S, Inoue I, Kawagoe T, Ishihara M, Shimatani Y, Nakama Y, Maruhashi T, Kagawa E, Dai K, Matsushita J, Ikenaga H. Prevalence of incidental coronary artery disease in tako-tsubo cardiomyopathy. Coron Artery Dis. 2009. 20:214–218.
Article9. Winchester DE, Ragosta M, Taylor AM. Concurrence of angiographic coronary artery disease in patients with apical ballooning syndrome (takotsubo cardiomyopathy). Catheter Cardiovasc Interv. 2008. 72:612–616.
Article10. Jie BS, Her SH, Yoon HJ, Jeong HB, Park CH, Jeon JH, Kwak JW, Kim YC, Lee SJ, Jin SW. A case of ST-segment elevation myocardial infarction mimicking stress-induced cardiomyopathy. J Cardiovasc Ultrasound. 2008. 16:29–32.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of ST-Segment Elevation Myocardial Infarction Mimicking Stress-Induced Cardiomyopathy
- A Case of Apical Hypertrophic Cardiomyopathy Combined Acute Myocardial Infarction with Multiple Coronary Thrombosis
- Reciprocal ST-segment depression in acute inferior myocardial infarction : Possible indicator of concomitant left anterior descending coronary artery stenosis
- Simultaneous Total Occlusion of Multiple Distal Coronary Arteries in Acute Myocardial Infarction
- Acute Coronary Syndrome Mimicking Atypical Stress-Induced Cardiomyopathy in a Patient with Panhypopituitarism
