Dependent Lung Opacity at Thin-Section CT: Evaluation by Spirometrically-Gated CT of the Influence of Lung Volume
- Affiliations
-
- 1Department of Diagnostic Radiology, Dong-A University College of Medicine, Pusan, Korea. kinamlee@chollian.net
- 2Department of Internal Medicine, Dong-A University College of Medicine, Pusan, Korea.
- 3Department of Thoracic Surgery, Dong-A University College of Medicine, Pusan, Korea.
- 4Department of Radiology, University of California, San Francisco.
- KMID: 1758443
- DOI: http://doi.org/10.3348/kjr.2002.3.1.24
Abstract
OBJECTIVE
To evaluate the influence of lung volume on dependent lung opacity seen at thin-section CT.
MATERIALS AND METHODS
In thirteen healthy volunteers, thin-section CT scans were performed at three levels (upper, mid, and lower portion of the lung) and at different lung volumes (10, 30, 50, and 100% vital capacity), using spirometric gated CT. Using a three-point scale, two radiologists determined whether dependent opacity was present, and estimated its degree. Regional lung attenuation at a level 2 cm above the diaphragm was determined using semiautomatic segmentation, and the diameter of a branch of the right lower posterior basal segmental artery was measured at each different vital capacity.
RESULTS
At all three anatomic levels, dependent opacity occurred significantly more often at lower vital capacities (10, 30%) than at 100% vital capacity (p = 0.001). Visually estimated dependent opacity was significantly related to regional lung attenuation (p < 0.0001), which in dependent areas progressively increased as vital capacity decreased (p < 0.0001). The presence of dependent opacity and regional lung attenuation of a dependent area correlated significantly with increased diameter of a segmental arterial branch (r = 0.493 and p = 0.0002; r = 0.486 and p = 0.0003, respectively).
CONCLUSION
Visual estimation and CT measurements of dependent opacity obtained by semiautomatic segmentation are significantly influenced by lung volume and are related to vascular diameter.
MeSH Terms
Figure
-
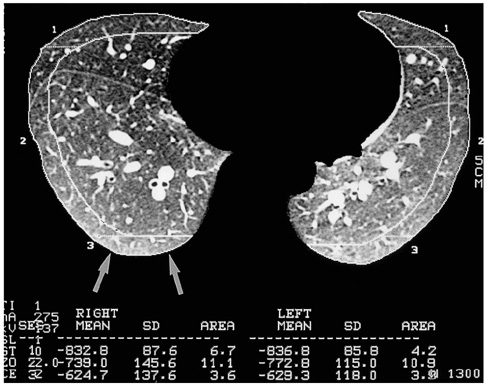
Fig. 1 The region of interest for measurements of regional lung attenuation was determined as a zone of the right lung posterior to a horizontal line drawn 1 cm from the most dependent lung. For the measurement of regional lung attenuation, we selected the same area (3.6 ± 0.6 cm2) as the most dependent area of a crescent shape (arrows).
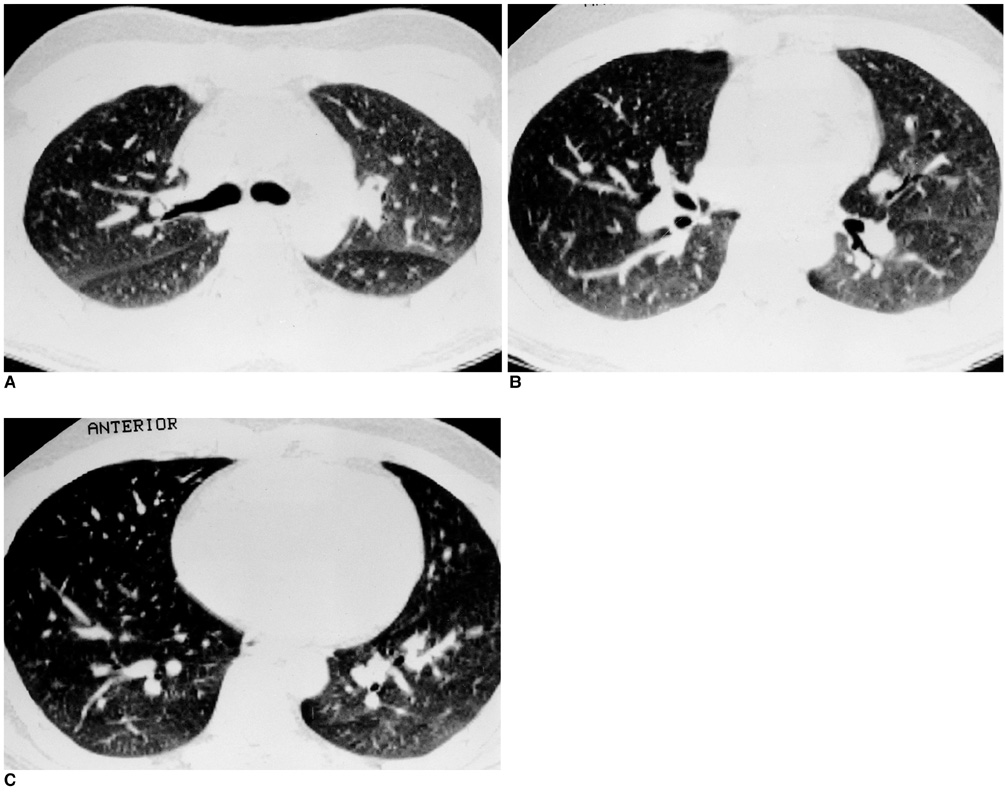
Fig. 2 Thirty-year-old man who showed dependent opacity (grade 2) at 10% vital capacity. A. Dependent opacity occurred at the level of the carina. Lung attenuation is greater in the posterior aspect of the upper lobes than in the superior segment of the lower lobes, located more posteriorly. Thus, dependent opacity is influenced not only by gravitational effects. B. Dependent opacity is seen at the level of the inferior pulmonary vein. C. Dependent opacity is prominent at a level 2 cm above the diaphragm.

Fig. 3 Comparison of dependent opacity and arterial diameter in a 29-year-old man A. Dependent opacity was obvious (grade 2) at 10% of vital capacity, and arterial diameter in the right posterior basal segment was 7.1 mm (artery, arrow). B. At 30% of vital capacity, dependent opacity was graded as subtle (grade 1) and arterial diameter measured 6.8 mm (arrow). C. Dependent opacity was not apparent at 50% of vital capacity (score 0), at which point arterial diameter was 6.6 mm (arrow). D. Dependent opacity was absent at 100% vital capacity, and at the same level, arterial diameter was 6.3 mm (arrow).
Reference
-
1. Webb WR, Muller NL, Naidich DP. An illustrated glossary of HRCT. High-resolution CT of the lung. 1996. 2nd ed. Philadelphia: Lippincott-Raven;295–311.2. Primack SL, Remy-Jardin M, Remy J, Muller NL. High-resolution CT of the lungs: pitfalls in the diagnosis of infiltrative lung disease. AJR. 1996. 167:413–418.3. Aberle DR, Gamsu G, Ray CS, Feuerstein IM. Asbestos-related pleural and parenchymal fibrosis: detection with high-resolution CT. Radiology. 1988. 166:729–734.4. Volpe J, Storto ML, Lee K, Webb WR. High-resolution CT of the lung: determination of the usefulness of CT scans obtained with the patient prone based on plain radiographic findings. AJR. 1997. 169:369–374.5. Hedlund LW, Vock P, Effmann EL. Evaluating lung density by computed tomography. Semin Respir Med. 1983. 5:76–88.6. Rosenblum LJ, Mauceri RA, Wellenstein DE, Bassano DA, Cohen WN, Heitzman ER. Density patterns in the normal lung as determined by computed tomography. Radiology. 1980. 137:409–416.7. Tokics L, Hedenstierna G, Strandberg A, Brismar B, Lundquist H. Lung collapse and gas exchange during general anesthesia: effects of spontaneous breathing, muscle paralysis and positive end-expiratory pressure. Anesthesiology. 1987. 66:157–167.8. Verschakelen JA, Van Fraeyenhoven L, Laureys G, Demedts M, Baert AL. Differences in CT density between dependent and nondependent portions of the lung: influence of lung volume. AJR. 1993. 161:713–717.9. Kalender WA, Rienmuller R, Seissler W, Behr J, Welke M, Fichte H. Measurement of pulmonary parenchymal attenuation: use of spirometric gating with quantitive CT. Radiology. 1990. 175:265–268.10. Rienmuller RK, Behr J, Kalender WA, et al. Standardized quantitative high-resolution CT in lung diseases. J Comput Assist Tomogr. 1991. 15:742–749.11. Kalender WA, Fichte H, Bautz W, Skalej M. Semiautomatic evaluation procedures for quantitative CT of the lung. J Comput Assist Tomogr. 1991. 15:248–255.12. Gevenois PA, Scillia P, de Maertelaer V, Michils A, Vuyst PD, Yernault J. The effects of age, sex, lung size and hyperinflation on CT lung densitometry. AJR. 1996. 167:1169–1173.13. Wegner OH, Koeppe P, Oeser H. Measurement of lung density by computed tomography. J Comput Assist Tomogr. 1978. 2:263–273.14. Wandtke JC, Hyde RW, Fahey PJ, et al. Measurement of lung gas volume and regional density by computed tomography in dogs. Invest Radiol. 1986. 21:108–117.15. Kohz P, Stabler A, Beinert T, et al. Reproducibility of quantitative, spirometrically controlled CT. Radiology. 1995. 197:539–542.16. Coxon HO, Mayo JR, Behzad H, et al. Measurement of lung expansion with computed tomography and comparison with quantitative histology. J Appl Physiol. 1995. 79:1525–1530.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Manifestations of Fat Embolism on Thin-section CT: A Case Report
- Cystic Lung Changes in a Thin Section CT in an Asymptomatic Young Adult with Unilateral Pulmonary Vein Atresia: A Case Report
- Mosaic Pattern of Lung Attenuation on Thin-Section CT: Review of 31 Cases
- Squalene Aspiration Pneumonia: Thin-Section CT and Histopathologic Findings
- The Effect of Lung Volume on the Size and Volume of Pulmonary Subsolid Nodules on CT: Intraindividual Comparison between Total Lung Capacity and Tidal Volume
