J Korean Surg Soc.
2009 Jun;76(6):348-354. 10.4174/jkss.2009.76.6.348.
Clinicopathologic Findings of Micropapillary Carcinomas, according to Tumor Size
- Affiliations
-
- 1Department of Surgery, College of Medicine, Chosun University, Gwangju, Korea. mdkckim8@hanmail.net
- KMID: 1464949
- DOI: http://doi.org/10.4174/jkss.2009.76.6.348
Abstract
-
PURPOSE: Papillary thyroid microcarcinomas (PTMC), which are not palpable and have no clinical symptoms are 1.0 cm or less in diameter. The optimal extent of thyroid tumor resection has been controversial. We investigated clinicopathological findings of PTMC of 5 mm or less in diameter for reasonable therapeutic approach.
METHODS
From, Jan. 2002 to Dec. 2006, 366 patients underwent thyroidectomy for thyroid papillary carcinoma at our institution. Among these patients, 62 patients with a mass measuring less than 5 mm and 103 patients with a mass 5 mm to 1.0 cm were selected. We retrospectively reviewed their medical records.
RESULTS
There was no significant difference on the clinical characteristics except multifocality. We performed more unilateral lobectomy, near total thyroidectomy with or without neck node dissection in patients with PTMC of less than 5 mm (P=0.13). In permanent biopsy, lymph node metastasis more frequently occurred in patients with PTMC of less than 5 mm (P=0.03). There were no differences in capsular invasion, distant metastasis or recurrence.
CONCLUSION
In papillary thyroid microcarcinoma less than 0.5 cm, it is very uncommon for capsular invasion, distant metastasis and locoregional metastasis to exist. The extent of tumor resection may be limited less than near total thyroidectomy for suitable cases, because there was no locoregional metastasis or distant metastasis in the follow-up period. Longer follow-up periods would be required to confirm that limited surgery is sufficient for tumors less than 0.5 cm in size.
MeSH Terms
Figure
-
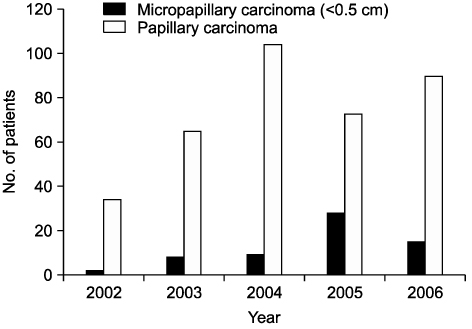
Fig. 1 The total number of papillary carcinoma and micropapillary carcinoma.
Cited by 1 articles
-
Clinical Significance of Tumor Size in Papillary Thyroid Microcarcinoma: a Meta-Analysis
Su-jin Kim, Kyungsik Kim, Young peck Song, Ho Kyung Sung, Kyu Eun Lee, Sue K. Park
J Endocr Surg. 2018;18(2):142-154. doi: 10.16956/jes.2018.18.2.142.
Reference
-
1. Gharib H. Fine-needle aspiration biopsy of thyroid nodules: advantages, limitations, and effect. Mayo Clin Proc. 1994. 69:44–49.2. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994. 97:418–428.3. Hedinger C, Williams ED, Sobin LH. The WHO histological classification of thyroid tumors: a commentary on the second edition. Cancer. 1989. 63:908–911.4. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004. 54:8–29.5. Pearce EN, Braverman LE. Papillary thyroid microcarcinoma outcomes and implications for treatment. J Clin Endocrinol Metab. 2004. 89:3710–3712.6. Gerrard G, Gill V. Thyroid cancer guidelines--what's new? Clin Oncol (R Coll Radiol). 2008. 20:264–266.7. Harach HR, Franssila KO. Occult papillary carcinoma of the thyroid appearing as lung metastasis. Arch Pathol Lab Med. 1984. 108:529–530.8. Falvo L, D'Ercole C, Sorrenti S, D'Andrea V, Catania A, Berni A, et al. Papillary microcarcinoma of the thyroid gland: analysis of prognostic factors including histological subtype. Eur J Surg Suppl. 2003. 28–32.9. Wada N, Duh QY, Sugino K, Iwasaki H, Kameyama K, Mimura T, et al. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003. 237:399–407.10. Jeon CH, Hong SM, Park JH, Paik SM, Jeong MH, Bong JG. The usefulness of preoperative ultrasonography on decision of operative extent in patients with papillary thyroid microcarcinoma. Korean J Endocrine Surg. 2006. 6:68–76.11. Kim JH, Yang JH. Papillary microcarcinoma of the thyroid. J Korean Surg Soc. 2001. 61:485–490.12. Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K, et al. Papillary microcarcinoma of the thyroid: how should it be treated? World J Surg. 2004. 28:1115–1121.13. Asanuma K, Kobayashi S, Shingu K, Hama Y, Yokoyama S, Fujimori M, et al. The rate of tumour growth does not distinguish between malignant and benign thyroid nodules. Eur J Surg. 2001. 167:102–105.14. Gooding GA. Sonography of the thyroid and parathyroid. Radiol Clin North Am. 1993. 31:967–989.15. Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997. 126:226–231.16. Brooks AD, Shaha AR, DuMornay W, Huvos AG, Zakowski M, Brennan MF, et al. Role of fine-needle aspiration biopsy and frozen section analysis in the surgical management of thyroid tumors. Ann Surg Oncol. 2001. 8:92–100.17. Haymart MR, Greenblatt DY, Elson DF, Chen H. The role of intraoperative frozen section if suspicious for papillary thyroid cancer. Thyroid. 2008. 18:419–423.18. Basolo F, Ugolini C, Proietti A, Iacconi P, Berti P, Miccoli P. Role of frozen section associated with intraoperative cytology in comparison to FNA and FS alone in the management of thyroid nodules. Eur J Surg Oncol. 2007. 33:769–775.19. Ito Y, Uruno T, Nakano K, Takamura Y, Miya A, Kobayashi K, et al. An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid. 2003. 13:381–387.20. Harach HR, Franssila KO, Wasenius VM. Occult papillary carcinoma of the thyroid. A "normal" finding in Finland. A systematic autopsy study. Cancer. 1985. 56:531–538.21. Kasai N, Sakamoto A. New subgrouping of small thyroid carcinomas. Cancer. 1987. 60:1767–1770.22. Pelizzo MR, Boschin IM, Toniato A, Piotto A, Bernante P, Pagetta C, et al. Papillary thyroid microcarcinoma (PTMC): prognostic factors, management and outcome in 403 patients. Eur J Surg Oncol. 2006. 32:1144–1148.23. Roti E, Rossi R, Trasforini G, Bertelli F, Ambrosio MR, Busutti L, et al. Clinical and histological characteristics of papillary thyroid microcarcinoma: results of a retrospective study in 243 patients. J Clin Endocrinol Metab. 2006. 91:2171–2178.24. Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH. Papillary microcarcinoma of the thyroid-Prognostic significance of lymph node metastasis and multifocality. Cancer. 2003. 98:31–40.25. Hay ID, Grant CS, van Heerden JA, Goellner JR, Ebersold JR, Bergstralh EJ. Papillary thyroid microcarcinoma: a study of 535 cases observed in a 50-year period. Surgery. 1992. 112:1139–1146.26. Cappelli C, Castellano M, Braga M, Gandossi E, Pirola I, De Martino E, et al. Aggressiveness and outcome of papillary thyroid carcinoma (PTC) versus microcarcinoma (PMC): a mono-institutional experience. J Surg Oncol. 2007. 95:555–560.27. Baudin E, Travagli JP, Ropers J, Mancusi F, Bruno-Bossio G, Caillou B, et al. Microcarcinoma of the thyroid gland: the Gustave-Roussy Institute experience. Cancer. 1998. 83:553–559.28. Haigh PI, Urbach DR, Rotstein LE. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol. 2005. 12:81–89.29. Shaha AR, Tuttle RM, Shah JP. Papillary microcarcinoma of the thyroid. J Surg Oncol. 2007. 95:532–533.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Micropapillary Carcinoma of the Breast: A clinicopathologic study of 16 cases
- Analysis of Clinicopathologic Factors Associated with Bilateral Thyroid Micro Papillary Carcinoma
- Micropapillary Carcinoma of Breast
- Prognostic Significance of a Micropapillary Pattern in Pure Mucinous Carcinoma of the Breast: Comparative Analysis with Micropapillary Carcinoma
- Invasive Micropapillary Carcinoma of the Breast: Mammographic, Sonographic and MR Imaging Findings
