Bisphosphonate related osteonecrosis of the jaws: report of two cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology and Research Institute of Oral Science, College of Dentistry, Gangneung-Wonju National University, Gangneung, Korea. hanjw@gwnu.ac.kr
- KMID: 1449958
- DOI: http://doi.org/10.5624/isd.2011.41.3.129
Abstract
- Bisphosphonates are compounds used to treat osteoporosis and malignant bone metastasis. Despite the benefits related to the use of these medications, osteonecrosis of the jaws is a significant complication in a subset of patients receiving these drugs. This complication occurs either spontaneously or after a simple dento-alveolar surgery. Recently there were two patients who showed the features of bisphosphonate related osteonecrosis of the jaws (BRONJ) in Gangneung-Wonju National University Dental Hospital. The patients revealed the clinical and radiological features of classical osteomyelitis. This report presents two cases of BRONJ which were examined by plain radiography and computed tomography.
MeSH Terms
Figure
-
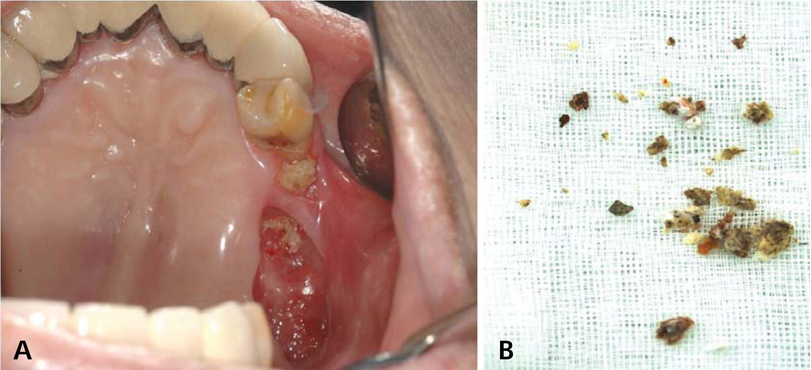
Fig. 1 Intraoral examination reveals alveolar bone exposure (A) and detached sequestrum (B) on left maxillary area of case 1.

Fig. 2 Panoramic radiograph shows a large osseous crater on left maxillary edentulous area.
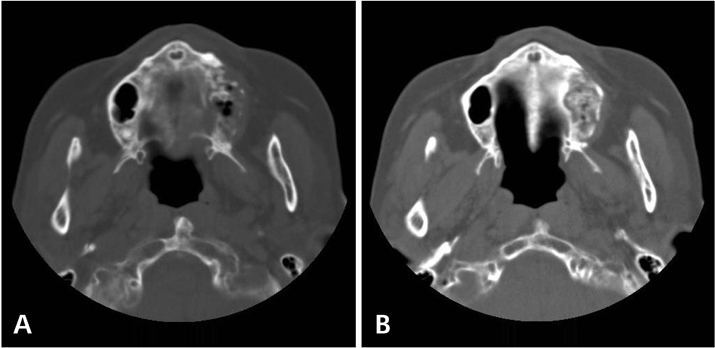
Fig. 3 A. Axial CT image reveals cortical bone destruction, sclerotic change of adjacent trabecular bone. B. Axial CT image reveals numerous bony fragments that is considered as sequestrum.

Fig. 4 Saucerization and decortication are performed on that area with sequestrectomy.
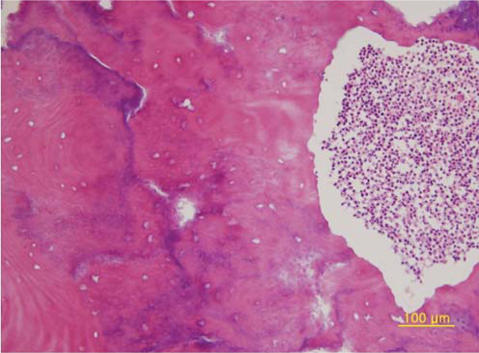
Fig. 5 Photomicrograph of specimen of biopsy shows infiltration of chronic inflammatory cell and no vivid osteocyte in the lacunae (H&E stain, ×200).

Fig. 6 Panoramic radiograph shows bone remodeling on the 6 months follow-up period in case 1. There is no sign of recurrence on left maxillary area.

Fig. 7 A. Intraoral radiograph of case 2 reveals bony fragment with trabeculation on socket of left maxillary canine. B. Panoramic radiograph shows separated lamina dura on socket of left maxillary canine.
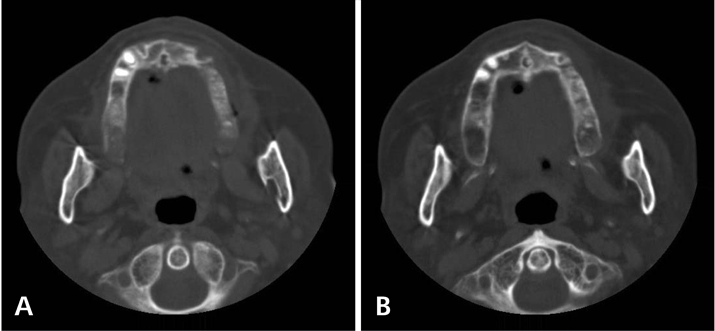
Fig. 8 A. Axial CT image reveals separated lamina dura on socket of left maxillary canine. B. Axial CT image shows mild buccal soft tissue swelling.

Fig. 9 Intraoral examination of case 2 reveals recurrence sign of alveolar bone exposure and pus discharge on right mandibular edentulous area.

Fig. 10 Panoramic radiograph shows decreased bone density and sequestrum on right mandibular area.

Fig. 11 Photomicrograph of sequestrum shows heavy infiltration of chronic inflammatory cell and bacterial flora (H&E stain, ×200).
Reference
-
1. Ruggiero SL, Fantasia J, Carlson E. Bisphosphonate-related osteonecrosis of the jaw: background and guidelines for diagnosis, staging and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006. 102:433–441.
Article2. Kos M, Kuebler JF, Luczak K, Engelke W. Bisphosphonate-related osteonecrosis of the jaws: a review of 34 cases and evaluation of risk. J Craniomaxillofac Surg. 2010. 38:255–259.
Article3. Magopoulos C, Karakinaris G, Telioudis Z, Vahtsevanos K, Dimitrakopoulos I, Antoniadis K, et al. Osteonecrosis of the jaws due to bisphosphonate use. A review of 60 cases and treatment proposals. Am J Otolaryngol. 2007. 28:158–163.
Article4. Lehrer S, Montazem A, Ramanathan L, Pessin-Minsley M, Pfail J, Stock RG, et al. Normal serum bone markers in bisphosphonate-induced osteonecrosis of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008. 106:389–391.
Article5. Campisi G, Di Fede O, Musciotto A, Lo Casto A, Lo Muzio L, Fulfaro F, et al. Bisphosphonate-related osteonecrosis of the jaw (BRONJ): run dental management designs and issues in diagnosis. Ann Oncol. 2007. 18:Suppl 6. vi168–vi172.
Article6. Morag Y, Morag-Hezroni M, Jamadar DA, Ward BB, Jacobson JA, Zwetchkenbaum SR, et al. Bisphosphonate-related osteonecrosis of the jaw: a pictorial review. Radiographics. 2009. 29:1971–1984.
Article7. Ruggiero SL. Bisphosphonate-related osteonecrosis of the jaw: an overview. Ann N Y Acad Sci. 2011. 1218:38–46.
Article8. Ficarra G, Beninati F. Bisphosphonate-related osteonecrosis of the jaws: an update on clinical, pathological and management aspects. Head Neck Pathol. 2007. 1:132–140.
Article9. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003. 61:1115–1117.
Article10. Ortega C, Montemurro F, Faggiuolo R, Vormola R, Nanni D, Goia F, et al. Osteonecrosis of the jaw in prostate cancer patients with bone metastases treated with zoledronate: a retrospective analysis. Acta Oncol. 2007. 46:664–668.
Article11. Conte-Neto N, Bastos AS, Spolidorio LC, Marcantonio RA, Marcantonio E Jr. Oral bisphosphonate-related osteonecrosis of the jaws in rheumatoid arthritis patients: a critical discussion and two case reports. Head Face Med. 2011. 7:7.
Article12. Abughazaleh K, Kawar N. Osteonecrosis of the jaws: what the physician needs to know: practical considerations. Dis Mon. 2011. 57:231–241.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multidisciplinary approach for medication-related osteonecrosis of the jaws: a case report and literature review
- Reconstruction of Defect after Treatment of Bisphosphonate-related Osteonecrois of the Jaw with Staged Iliac Bone Graft
- Radiologic Findings of Oral Bisphosphonate-Related Osteonecrosis of the Maxilla, Complicated by Actinomycosis: A Case Report
- Oral Bisphosphonate Related Osteonecrosis of the Jaws: A case report
- Osteonecrosis of the Jaw in Korean Woman with Osteoporosis Treated with Oral Bisphosphonate: Case Report
