Radiologic Findings of Oral Bisphosphonate-Related Osteonecrosis of the Maxilla, Complicated by Actinomycosis: A Case Report
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea. hyungkim@skku.edu
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- 3Department of Oral and Maxillofacial Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- KMID: 2208989
- DOI: http://doi.org/10.3348/jksr.2010.62.1.17
Abstract
- Bisphosphonate-related osteonecrosis of the jaw (BRONJ) is a rare, but serious complication, which has recently been more frequently reported. However, this entity is unfamiliar to radiologists. We report a case of BRONJ complicated by actinomycosis following a tooth extraction in a 68-year-old woman who has been treated with oral bisphosphonate for treatment of osteoporosis over the last 3 years and 3 months.
MeSH Terms
Figure
-
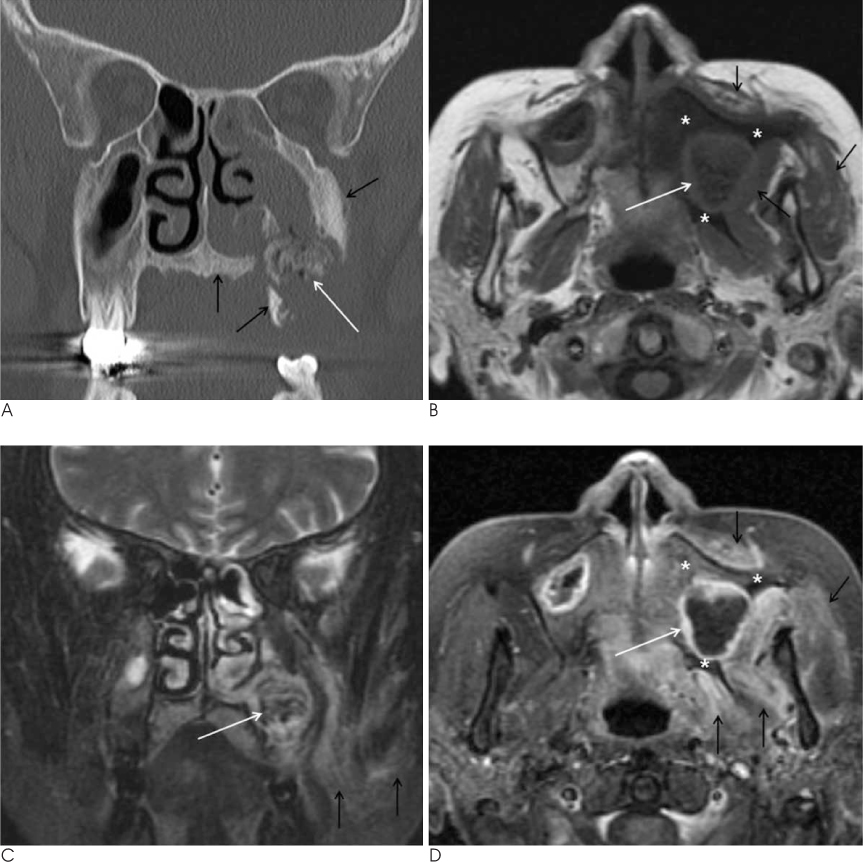
Fig. 1 Bisphophonate-related osteonecrosis of the maxilla complicated by actinomycosis in a 66-year-old woman. A. Coronal CT scan with bone algorithm shows irregular destruction of the alveolar bone of the left posterior maxilla. There is a large sequestrum at the area of destroyed left maxillary sinus floor, manifesting as an irregular, laminated, fragmented bone containing the mottled air densities (white arrow). Ipsilateral maxillary and ethmoid sinuses as well as the nasal cavity are opacified by the inflammatory tissues. Note the sclerotic change of the adjacent bones (black arrows). B-D. Axial T1-weighted (B), coronal fat-suppressed T2-weighted (C), and axial contrast-enhanced fat-suppressed T1-weighted (D) MR images nicely show the findings of sequestrum, osteosclerosis, and inflammatory infiltrates to the deep neck spaces. The sequestrum shows diffuse low signal intensity on T1-weighted image, heterogeneous signal intensity on T2-weighted image (white arrows), and no significant enhancement on contrast-enhanced image, and is surrounded by the inflammatory tissue which shows isointensity on T1-weighted image, hyperintensity on T2-weighted image, and intense enhancement on contrast-enhanced image. Osteosclerosis of the adjacent bone is seen as diffuse hypointense signal on T1-weighted image, diffuse hyperintense signal on T2-weighted image, and diffuse moderate enhancement on contrast-enhanced image (asterisks), indicating the associated bone marrow infection (osteomyelitis). There is extensive soft tissue infiltration into the infratemporal fossa as well as the anterior cheek due to the spread of infection, which manifests as isointensity on T1-weighted image, hyperintensity on T2-weighted image, and moderate enhancement on contrast-enhanced image (black arrows).
Reference
-
1. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003; 61:1115–1117.2. Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, Mehrotra B. American association of oral and maxillofacial surgeons position paper on bisphosphonate-related osteonecrosis of the jaws-2009 Update. J Oral Maxillofac Surg. 2009; 67:5 Suppl 1. 2–12.3. Hansen T, Kunkel M, Springer E, Walter C, Weber A, Siegel E, et al. Actinomycosis of the jaws-histopathological study of 45 patients shows significant involvement in bisphosphonate-associated osteonecrosis and infected osteoradionecrosis. Virchows Arch. 2007; 451:1009–1017.4. Woo SB, Hellstein JW, Kalmar JR. Narrative [corrected] review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006; 144:753–761.5. Phal PM, Myall RW, Assael LA, Weissman JL. Imaging findings of bisphosphonate-associated osteonecrosis of the jaws. AJNR Am J Neuroradiol. 2007; 28:1139–1145.6. Arce K, Assael LA, Weissman JL, Markiewicz MR. Imaging findings in bisphosphonate-related osteonecrosis of jaws. J Oral Maxillofac Surg. 2009; 67:5 suppl. 75–84.7. Bisdas S, Chambron Pinho NC, Smolarz A, Sader R, Vogl TJ, Mack MG. Biphosphonate-induced osteonecrosis of the jaws: CT and MRI spectrum of findings in 32 patients. Clin Radiol. 2008; 63:71–77.8. Bianchi SD, Scoletta M, Cassione FB, Migliaretti G, Mozzati M. Computerized tomographic findings in bisphosphonate-associated osteonecrosis of the jaw in patients with cancer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104:249–258.9. Bedogni A, Blandamura S, Lokmic Z, Palumbo C, Ragazzo M, Ferrari F, et al. Bisphosphonate-associated jawbone osteonecrosis: a correlation between imaging techniques and histopathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:358–364.10. Garcia-Ferrer L, Bagán JV, Martinez-Sanjuan V, Hernandez-Bazan S, Garcia R, Jiménez-Soriano Y, et al. MRI of mandibular osteonecrosis secondary to bisphosphonates. AJR Am J Roentgenol. 2008; 190:949–955.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Features of Histopathologic and radiographic findings in bisphosphonate-related osteonecrosis of jaw-Clinical review
- Oral Bisphosphonate Related Osteonecrosis of the Jaws: A case report
- Clinical feature and treatment of bisphosphonate-related osteonecrosis of jaw about oral bisphosphonate administrated patients: case reports
- Bisphosphonate-Related Osteonecrosis in a Patient with Florid Cemento-Osseous Dysplasia
- Bisphosphonate, is it an emerging risk factor in oral surgery?
