Spontaneous Complete Occlusion of Middle Cerebral Artery Aneurysm: Case Report
- Affiliations
-
- 1Department of Neurosurgery, Busan Paik Hospital, Inje university College of Medicine, Busan, Korea.
- 2Department of Neurosurgery, Haeundae Paik Hopspital, Inje university College of Medicine, Busan, Korea. nssunlee@inje.ac.kr
- KMID: 1431286
- DOI: http://doi.org/10.7461/jcen.2012.14.4.309
Abstract
- There are few observation papers regarding the natural history of an aneurysm. We report on a case of a completely occluded middle cerebral artery (MCA) aneurysm. A 47-year-old female patient presented with a headache and was diagnosed with rupture of a right MCA aneurysm. Due to a high risk of direct neck clipping, she received conservative treatment after craniotomy and wrapping of her aneurysm. The patient's condition showed improvement, with complete occlusion of the aneurysm and considerable reduction of the aneurysm in size after approximately three years. This is a rare case of an aneurysm of MCA that showed spontaneous resolution. Finally, on the angiogram, characteristics of an aneurysm to occlude spontaneously will be presumed based on literature reviews.
MeSH Terms
Figure
-

Fig. 1 (A) Axial computed tomography (CT) scan shows a slightly high-density intra axial mass lesion measuring approximately 2.5 cm, along the peripheral side of the right sylvian fissure. No edema was observed around the mass. There was no calcification either. (B) After contrast enhancement, the mass lesion showed significant enhancement. (C) Three-dimensional CT angiography reconstruction showing a saccular aneurysm in the right middle cerebral artery (MCA) bifurcation.
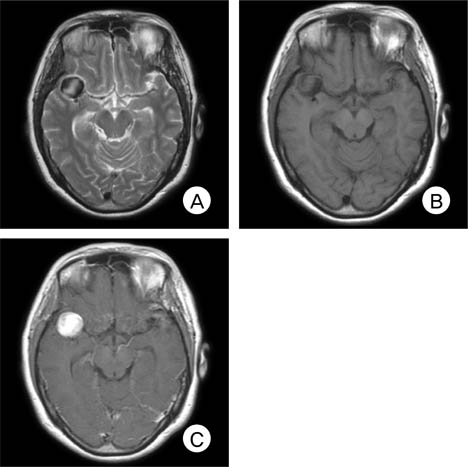
Fig. 2 (A) T2 weighted images from a brain magnetic resonance image (MRI) examination show a high signal in the aneurysm sac and a heterogeneous, peripheral low signal. (B) T1 weighted image shows a low signal in a portion close to the Circle of Willis and an iso signal far from it. (C) After contrast enhancement, strong improvement with a filling difference in the aneurysm sac is observed.
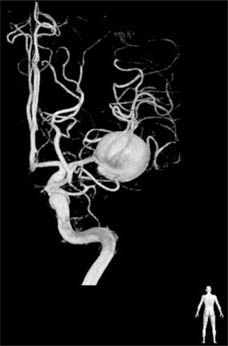
Fig. 3 Right internal carotid artery angiogram (three-dimensional subtraction image) posterior to anterior view. An aneurysm measuring 21.6 × 20.9 mm in the right MCA bifurcation is observed in a lateral direction, and an aneurysm of the right MCA bifurcation formed a broad neck along an inferior branch of M2. Several perforating branches are observed around the neck.
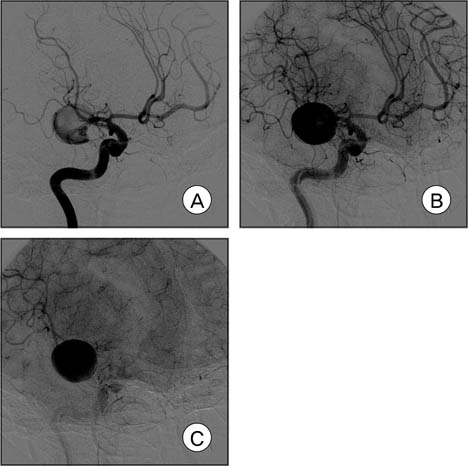
Fig. 4 Right internal carotid artery angiogram. Slow filling and delayed excretion pattern are noted (A, B and C).
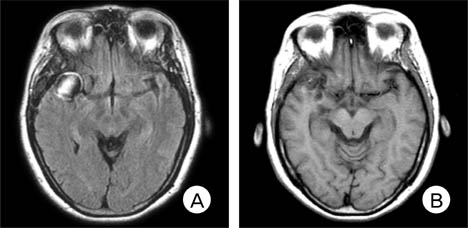
Fig. 5 (A) MRI obtained eight months later. A target sign that appeared as a high signal, a low signal in the slightly inner portion and a high signal again in the central portion, is seen on the T1 image around the aneurysm. (B) After 19 months, the size of the aneurysm shows a considerable decrease.
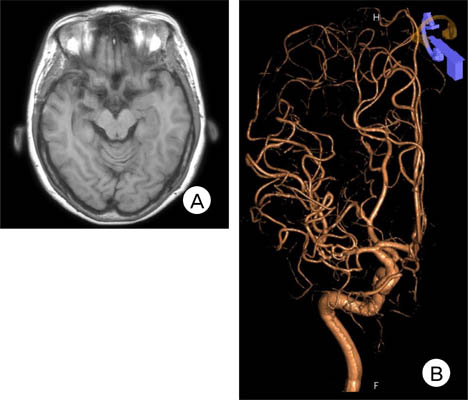
Fig. 6 (A) MRI obtained three years and eight months later, showing considerable reduction in the size of the aneurysm and no trace of the mass in the sylvian fissure. (B) Three-dimensional angiography reveals an occlusion of the aneurysm and intact M2 branches.
Cited by 1 articles
-
Thrombosis and Recanalization of Small Saccular Cerebral Aneurysm : Two Case Reports and a Suggestion for Possible Mechanism
Hyung Jun Kim, Jae Hoon Kim, Duk Ryung Kim, Hee In Kang
J Korean Neurosurg Soc. 2014;55(5):280-283. doi: 10.3340/jkns.2014.55.5.280.
Reference
-
1. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms-risk of rupture and risks of surgical intervention. N Engl J Med. 1998. 12. 339(24):1725–1733.2. De Lange SA. [A case of spontaneous thrombosis of a cerebral arteriovenous aneurysm]. Ned Tijdschr Geneeskd. 1955. 03. 99(13):944–946. Dutch.3. Vasconcellos LP, Flores JAC, Conti MLM, Veiga JCE, Lancellotti CLP. Spontaneous thrombosis of internal carotid artery: a natural history of giant carotid cavernous aneurysms. Arq Neuropsiquiatr. 2009. 06. 67(2A):278–283.
Article4. Deshmukh VR, Kakarla UK, Figueiredo EG, Zabramski JM, Spetzler RF. Long-term clinical and angiographic follow-up of unclippable wrapped intracranial aneurysms. Neurosurgery. 2006. 03. 58(3):434–442. discussion 434-42.
Article5. Fujiwara S, Fujii K, Nishio S, Fukui M. Long-term results of wrapping of intracranial ruptured aneurysms. Acta Neurochir (Wien). 1990. 103(1-2):27–29.6. Gerber S, Dormont D, Sahel M, Grob R, Foncin JF, Marsault C. Complete spontaneous thrombosis of a giant intracranial aneurysm. Neuroradiology. 1994. 05. 36(4):316–317.
Article7. Hay KL, Bull BS. Factors influencing the activation of platelets by nonionic contrast medium. J Vasc Interv Radiol. 1996. May-Jun. 7(3):401–407.
Article8. Heiskanen O. Risks of surgery for unruptured intracranial aneurysms. J Neurosurg. 1986. 10. 65(4):451–453.
Article9. Inagawa T. Surgical treatment of multiple intracranial aneurysms. Acta Neurochir (Wien). 1991. 108(1-2):22–29.
Article10. King JT Jr, Berlin JA, Flamm ES. Morbidity and mortality from elective surgery for asymptomatic, unruptured, intracranial aneurysms: a meta-analysis. J Neurosurg. 1994. 12. 81(6):837–842.
Article11. Krapf H, Schoning M, Petersen D, Kuker W. Complete asymptomatic thrombosis and resorption of a congenital giant intracranial aneurysm. J Neurosurg. 2002. 07. 97(1):184–189.
Article12. Loevner LA, Ting TY, Hurst RW, Goldberg HI, Schut L. Spontaneous thrombosis of a basilar artery traumatic aneurysm in a child. AJNR Am J Neuroradiol. 1998. 02. 19(2):386–388.13. Maruyama M, Asai T, Kuriyama Y, Sawada T, Ogata J, Nishimura T, et al. Positive platelet scintigram of a vertebral aneurysm presenting thromboembolic transient ischemic attacks. Stroke. 1989. 05. 20(5):687–690.
Article14. Moron F, Benndorf G, Akpek S, Dempsy R, Strother CM. Spontaneous thrombosis of a traumatic posterior cerebral artery aneurysm in a child. AJNR Am J Neuroradiol. 2005. 01. 26(1):58–60.15. Nakstad P. Spontaneous occlusion of traumatic pericallosal aneurysm and pericallosal artery. Neuroradiology. 1987. 29(3):312.
Article16. Sato K, Fujiwara S, Kameyama M, Ogawa A, Yoshimoto T, Suzuki J. Follow-up study on ruptured aneurysms treated by wrapping. Neurol Med Chir (Tokyo). 1990. 30(10):734–737.
Article17. Todd NV, Tocher JL, Jones PA, Miller JD. Outcome following aneurysm wrapping: a 10-year follow-up review of clipped and wrapped aneurysms. J Neurosurg. 1989. 06. 70(6):841–846.
Article18. Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms. Brain. 2000. 02. 123(Pt 2):205–221.
Article19. Whittle IR, Dorsch NW, Besser M. Spontaneous thrombosis in giant intracranial aneurysms. J Neurol Neurosurg Psychiatry. 1982. 11. 45(11):1040–1047.
Article20. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003. 07. 362(9378):103–110.
Article21. Yasargil MG, Vise WM, Bader DC. Technical adjuncts in neurosurgery. Surg Neurol. 1977. 8(5):331–336.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Distal Middle Cerebral Artery M4 Aneurysm Surgery Using Navigation-CT Angiography
- Duplication of the Middle Cerebral Artery: Case Report
- Ruptured Distal Lenticulostriate Artery Aneurysm Associated with Ipsilateral Middle Cerebral Artery Occlusion : Case Report
- Spontaneous Dissecting Aneurysm of the Anterior Cerebral Artery: Report of 2 Cases
- Ruptured Dissecting Aneurysm of the Middle Cerebral Artery with Spontaneous Resolution: A Case Report
