Strategies for Successful Percutaneous Revascularization of Chronic Total Occlusion of the Femoropopliteal Arteries When the Antegrade Passage of a Guide Wire Fails
- Affiliations
-
- 1Department of Radiology, Konkuk University Hospital, Konkuk University School of Medicine, Seoul 143-729, Korea. psw0224@kuh.ac.kr
- KMID: 1383859
- DOI: http://doi.org/10.3348/kjr.2012.13.4.467
Abstract
OBJECTIVE
To evaluate the efficacy of various strategies for revascularization of chronic total occlusion of femoropopliteal arteries when the guide wire does not pass in an anterograde direction.
MATERIALS AND METHODS
Twenty-four patients with totally occluded femoropopliteal arteries (mean occlusion length 13.75 cm; range, 6-22 cm) were treated by using a retrograde approach and two novel catheters. After successful recanalization or reentry, balloon angioplasty followed by stent placement was performed to complete the revascularization.
RESULTS
In 16 cases in which to cross the occlusion via intraluminal or subintimal route was failed, we used Frontrunner catheters in five cases and Outback catheters in 11 cases. In eight cases in which to reenter after subintimal passage of the guide wire was failed, we used Outback catheters. Successful recanalization was achieved intraluminally or subintimally in all cases. One perforation occurred during subintimal passage of the guide wire that was controlled by recanalization of another subintimal tract. There were no cases of distal thromboembolism or other complications.
CONCLUSION
A retrograde approach and using the Frontrunner and Outback catheters are safe and effective for successful revascularization of chronic total occlusion of femoropopliteal arteries. In particular, they are useful when the initial antegrade attempts at recanalization have failed.
MeSH Terms
Figure
-
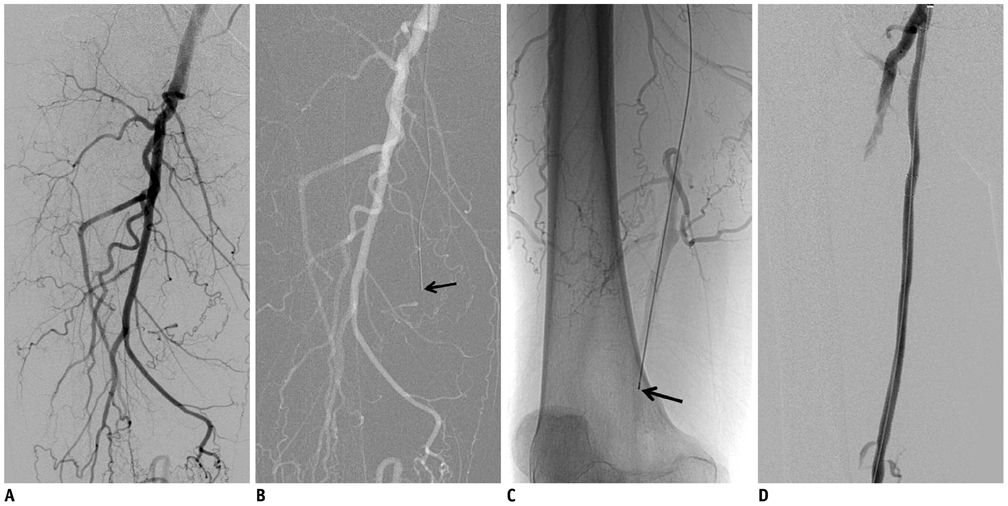
Fig. 1 64-year-old man with severe claudication (Fontaine classification IIb) of right leg. A-C. Patient had chronic total occlusion of about 20 cm of right superficial femoral artery on angiogram. Successful recanalization with Frontrunner XP chronic total occlusion catheter was achieved into reconstituted artery (arrow). D. Primary stent placement with self-expandable nitinol stents was performed.

Fig. 2 73-year-old man with severe claudication (Fontaine classification IIb) of both legs. A. Patient had chronic total occlusion of about 8 cm of left superficial femoral artery on angiogram (arrow). B. Reentry of 0.035 inch hydrophilic guide wire into true lumen could not be achieved. C, D. Under ultrasound guidance, popliteal arterial puncture was performed and chronic total occlusion lesion was crossed subinitmally in retrograde fashion. Anterograde snare was used to maneuver wire into sheath to facilitate subsequent procedures in anterograde manner. E. Thereafter, balloon angioplasty followed by stent placement was performed in femoropopliteal arteries and hemostasis in popliteal artery was established by manual compression.

Fig. 3 81-year-old-woman with severe claudication (Fontaine classification IIb) of left superficial femoral artery (SFA). A. Patient had chronic total occlusion of about 17 cm in left SFA on angiogram. B. Fluoroscopic images show Outback catheter and its needle deployed (double arrows) with free passage of guide wire into true lumen of reconstituted artery. L configuration at catheter nosecone is noted (arrow). C. Final angiogram demonstrates that patency was restored following stent placement.
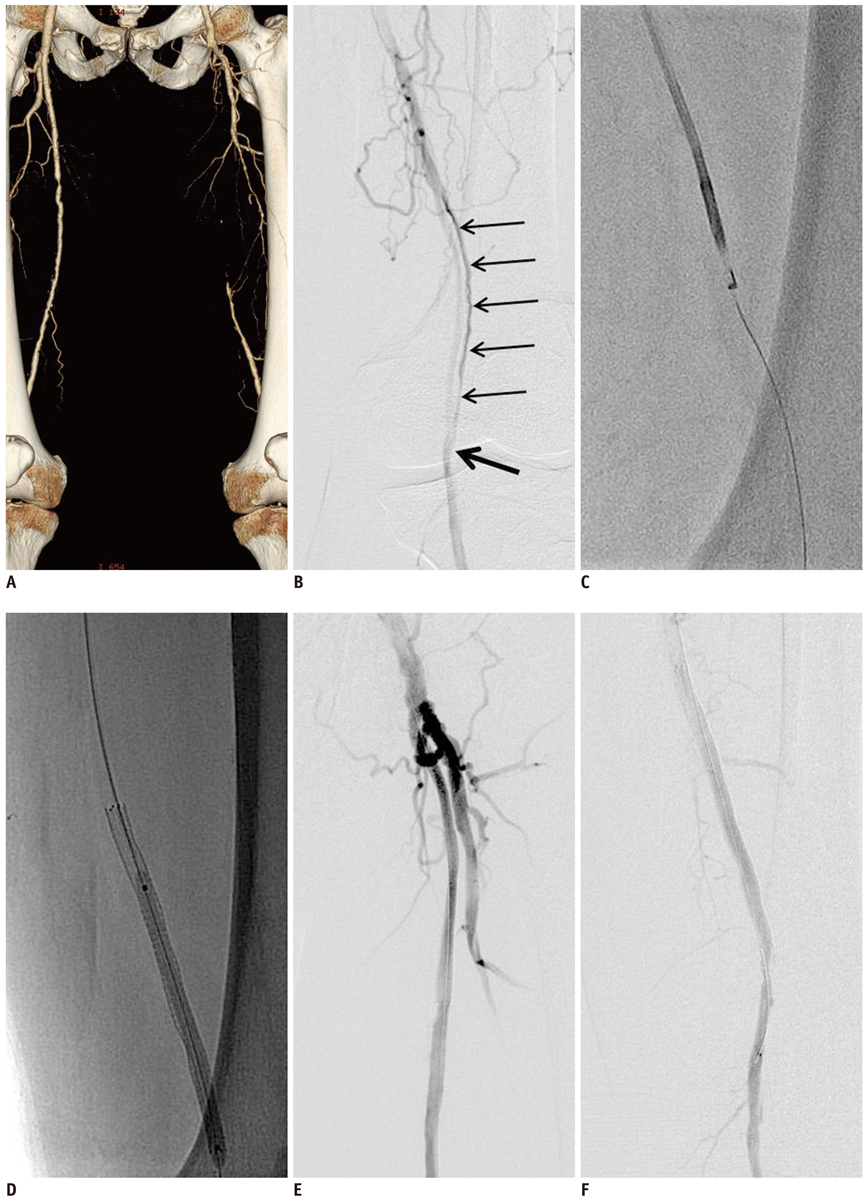
Fig. 4 71-year-old-man with resting pain (Fontaine classification III) in left foot. A. CT angiography shows chronic total occlusion of left superficial femoral artery (SFA). B. Initial attempt with conventional techniques using hydrophilic guide wire and angiographic catheter created reentry at P2 segment of popliteal artery (arrow). Angiogram after subintimal angioplasty showed suboptimal results (thin arrows). C. Outback catheter was used to create new reentry site at more proximal artery to P2 segment of popliteal artery to allow stent to be placed. D. Self-expandable nitinol stent was placed at distal SFA including new reentry site. E, F. Final angiogram demonstrates that patency was restored following stent placement.
Reference
-
1. Kjellgren O, Feld S, Loyd D, Schroth G, Anderson HV, Smalling RW. Successful treatment of chronic total peripheral occlusions that failed conventional techniques using the stiff backend of the Glidewire. Cathet Cardiovasc Diagn. 1995. 36:360–363.2. Gupta AK, Ravimandalam K, Rao VR, Joseph S, Unni M, Rao AS, et al. Total occlusion of iliac arteries: results of balloon angioplasty. Cardiovasc Intervent Radiol. 1993. 16:165–177.3. Bolia A, Miles KA, Brennan J, Bell PR. Percutaneous transluminal angioplasty of occlusions of the femoral and popliteal arteries by subintimal dissection. Cardiovasc Intervent Radiol. 1990. 13:357–363.4. Henry M, Amor M, Ethevenot G, Henry I, Mentre B, Tzvetanov K. Percutaneous endoluminal treatment of iliac occlusions: long-term follow-up in 105 patients. J Endovasc Surg. 1998. 5:228–235.5. van der Heijden FH, Eikelboom BC, Banga JD, Mali WP. Management of superficial femoral artery occlusive disease. Br J Surg. 1993. 80:959–963.6. Tønnesen KH, Sager P, Karle A, Henriksen L, Jørgensen B. Percutaneous transluminal angioplasty of the superficial femoral artery by retrograde catheterization via the popliteal artery. Cardiovasc Intervent Radiol. 1988. 11:127–131.7. Zaitoun R, Iyer SS, Lewin RF, Dorros G. Percutaneous popliteal approach for angioplasty of superficial femoral artery occlusions. Cathet Cardiovasc Diagn. 1990. 21:154–158.8. Heenan SD, Vinnicombe SJ, Buckenham TM, Belli AM. Percutaneous transluminal angioplasty by a retrograde subintimal transpopliteal approach. Clin Radiol. 1994. 49:824–827. discussion 827-828.9. Villas PA, Cohen G, Goyal A, Putnam SG 3rd, Ball D. The merits of percutaneous transluminal angioplasty of a superficial femoral artery stenosis via a retrograde popliteal artery approach. J Vasc Interv Radiol. 1999. 10:325–328.10. Yilmaz S, Sindel T, Ceken K, Alimoğlu E, Lüleci E. Subintimal recanalization of long superficial femoral artery occlusions through the retrograde popliteal approach. Cardiovasc Intervent Radiol. 2001. 24:154–160.11. Cutress ML, Blanshard K, Shaw M, Bown M, White S, Sayers RD. Retrograde subintimal angioplasty via a popliteal artery approach. Eur J Vasc Endovasc Surg. 2002. 23:275–276.12. Spinosa DJ, Harthun NL, Bissonette EA, Cage D, Leung DA, Angle JF, et al. Subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) for subintimal recanalization to treat chronic critical limb ischemia. J Vasc Interv Radiol. 2005. 16:37–44.13. Etezadi V, Benenati JF, Patel PJ, Patel RS, Powell A, Katzen BT. The reentry catheter: a second chance for endoluminal reentry at difficult lower extremity subintimal arterial recanalizations. J Vasc Interv Radiol. 2010. 21:730–734.14. London NJ, Srinivasan R, Naylor AR, Hartshorne T, Ratliff DA, Bell PR, et al. Subintimal angioplasty of femoropopliteal artery occlusions: the long-term results. Eur J Vasc Surg. 1994. 8:148–155.15. Yilmaz S, Sindel T, Lüleci E. Subintimal versus intraluminal recanalization of chronic iliac occlusions. J Endovasc Ther. 2004. 11:107–118.16. Conroy RM, Gordon IL, Tobis JM, Hiro T, Kasaoka S, Stemmer EA, et al. Angioplasty and stent placement in chronic occlusion of the superficial femoral artery: technique and results. J Vasc Interv Radiol. 2000. 11:1009–1020.17. Yilmaz S, Sindel T, Luleci E. Bilateral transpopliteal approach for treatment of complex SFA and iliac occlusions. Eur Radiol. 2002. 12:911–914.18. Wiesinger B, Steinkamp H, König C, Tepe G, Duda SH. Technical report and preliminary clinical data of a novel catheter for luminal re-entry after subintimal dissection. Invest Radiol. 2005. 40:725–728.19. Hausegger KA, Georgieva B, Portugaller H, Tauss J, Stark G. The outback catheter: a new device for true lumen re-entry after dissection during recanalization of arterial occlusions. Cardiovasc Intervent Radiol. 2004. 27:26–30.20. Ingle H, Nasim A, Bolia A, Fishwick G, Naylor R, Bell PR, et al. Subintimal angioplasty of isolated infragenicular vessels in lower limb ischemia: long-term results. J Endovasc Ther. 2002. 9:411–416.21. Lazaris AM, Tsiamis AC, Fishwick G, Bolia A, Bell PR. Clinical outcome of primary infrainguinal subintimal angioplasty in diabetic patients with critical lower limb ischemia. J Endovasc Ther. 2004. 11:447–453.22. Laxdal E, Jenssen GL, Pedersen G, Aune S. Subintimal angioplasty as a treatment of femoropopliteal artery occlusions. Eur J Vasc Endovasc Surg. 2003. 25:578–582.23. Smith BM, Stechman M, Gibson M, Torrie EP, Magee TR, Galland RB. Subintimal angioplasty for superficial femoral artery occlusion: poor patency in critical ischaemia. Ann R Coll Surg Engl. 2005. 87:361–365.24. Molloy KJ, Nasim A, London NJ, Naylor AR, Bell PR, Fishwick G, et al. Percutaneous transluminal angioplasty in the treatment of critical limb ischemia. J Endovasc Ther. 2003. 10:298–303.25. Hynes N, Akhtar Y, Manning B, Aremu M, Oiakhinan K, Courtney D, et al. Subintimal angioplasty as a primary modality in the management of critical limb ischemia: comparison to bypass grafting for aortoiliac and femoropopliteal occlusive disease. J Endovasc Ther. 2004. 11:460–471.26. Yang YM, Mehran R, Dangas G, Reyes A, Qin J, Stone GW, et al. Successful use of the frontrunner catheter in the treatment of in-stent coronary chronic total occlusions. Catheter Cardiovasc Interv. 2004. 63:462–468.27. Charalambous N, Schäfer PJ, Trentmann J, Hümme TH, Stöhring C, Muller-Hulsbeck S, et al. Percutaneous intraluminal recanalization of long, chronic superficial femoral and popliteal occlusions using the Frontrunner XP CTO device: a single-center experience. Cardiovasc Intervent Radiol. 2010. 33:25–33.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- Recanalization of a Coronary Chronic Total Occlusion by a Retrograde Approach Using Ipsilateral Double Guiding Catheters
- Interventional Management of “Balloon-Uncrossable†Coronary Chronic Total Occlusion: Is There Any Way Out?
- Endovascular Treatment of Multilevel Chronic Total Occlusion Using a Stent Puncture Technique in Buerger's Disease
- Dorsal-Plantar Loop Technique Using Chronic Total Occlusion Devices via Anterior Tibial Artery
