Interventional Management of “Balloon-Uncrossable†Coronary Chronic Total Occlusion: Is There Any Way Out?
- Affiliations
-
- 1Thumbay Hospital, Ajman, United Arab Emirates. dr_dash2003@yahoo.com
- 2Beijing Tiantan Hospital, Beijing, China.
- KMID: 2407897
- DOI: http://doi.org/10.4070/kcj.2017.0345
Abstract
- It has been estimated that coronary chronic total occlusion (CTO) is encountered in 15 to 20% patients referred for coronary angiography (CAG). The success of percutaneous coronary intervention (PCI) of CTO can be attributed to the vast array of hardware that has now become available and also to the vastly enhanced operator expertise. It is however realistic to state that despite the tremendous increase in the rate of success, there then comes a subset of CTO where PCI attempts fail. The reason for such failures given that other variables remain constant is the inability to cross the CTO lesion. This can be due to a failure to cross the lesion with a guide wire (despite guide wire escalation). The second cause of failure is the inability to cross the lesion with a balloon (balloon-uncrossable [BU] CTO). This can occur despite the successful placement of a guidewire in the distal true lumen. The BU lesions contribute 2% to 10% of CTO PCI failure cases. The author attempts to present a creative solution to assist crossing such lesions.
Figure
-
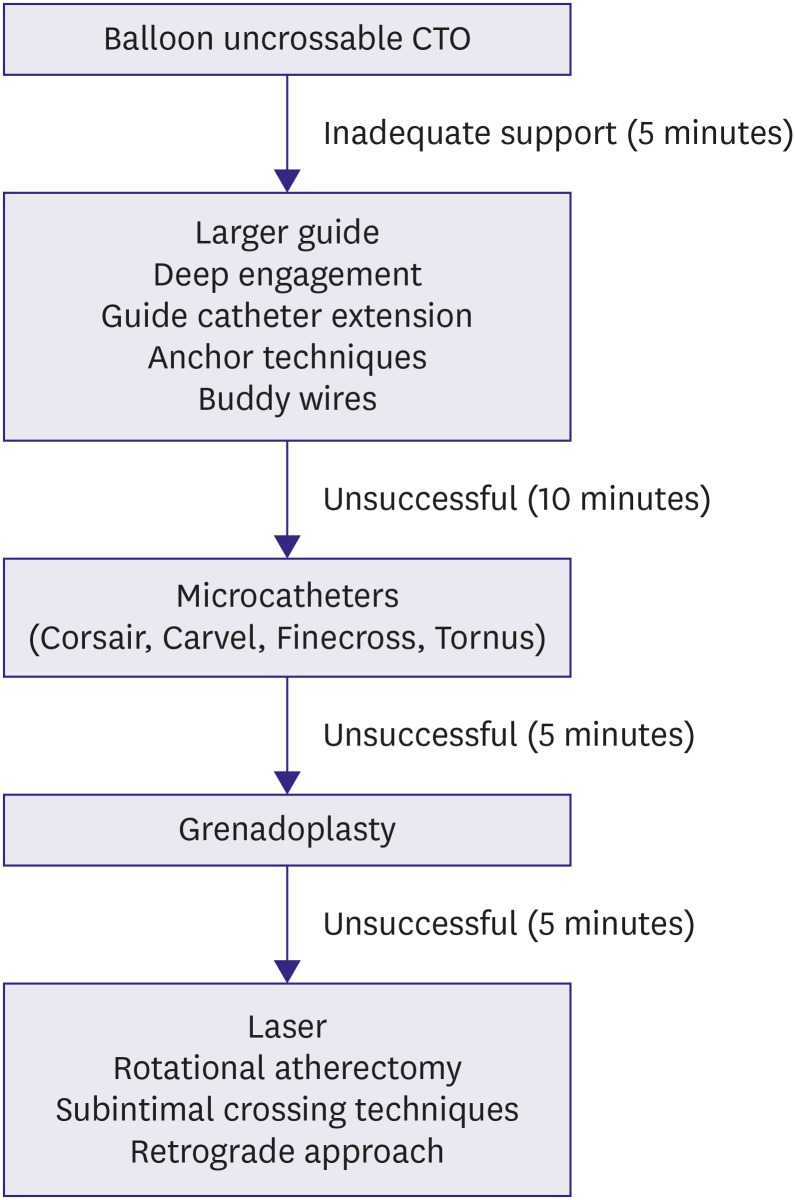
Figure 1 Algorithm for crossing a BU CTO.BU = balloon-uncrossable; CTO = chronic total occlusion.
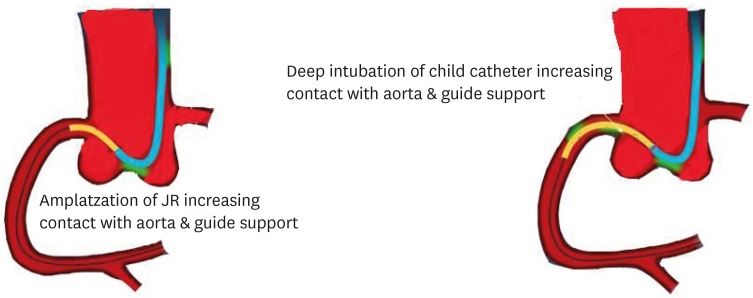
Figure 2 Schematic illustration of augmentation of guide catheter back up by guide extension catheter.
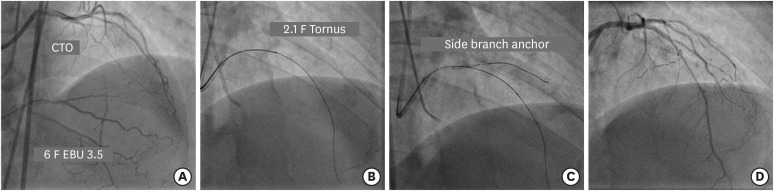
Figure 3 (A) Engagement of LMCA ostium with 6 F EBU 3.5 guide catheter to address long mid segment CTO of LAD artery. (B) Failure of 1.25×12 mm balloon to cross the lesion after insertion of Gaia 2 guidewire followed by navigation of 2.1 F Tornus catheter. (C) A 2×12 mm balloon in diagonal artery acts as an anchor. (D) Final result after deployment of 2 overlapping DES.CTO = chronic total occlusion; DES = drug-eluting stent; LAD = left anterior descending; LMCA = left main coronary artery.
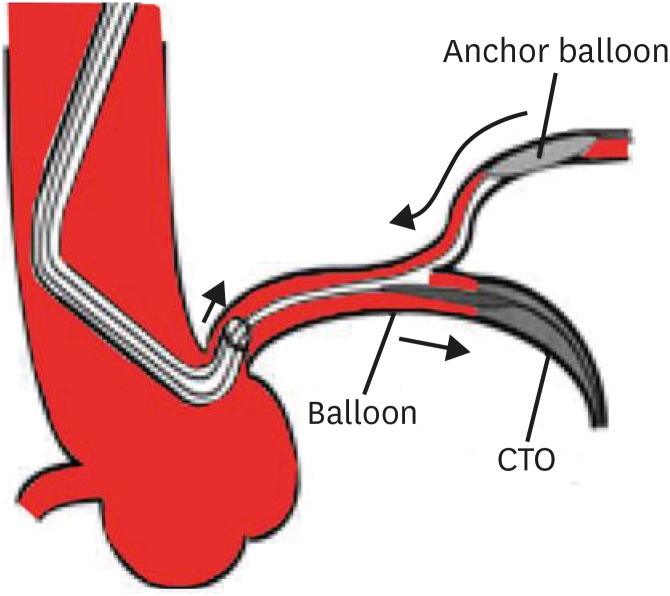
Figure 4 Schematic illustration of side branch anchor balloon technique.CTO = chronic total occlusion.
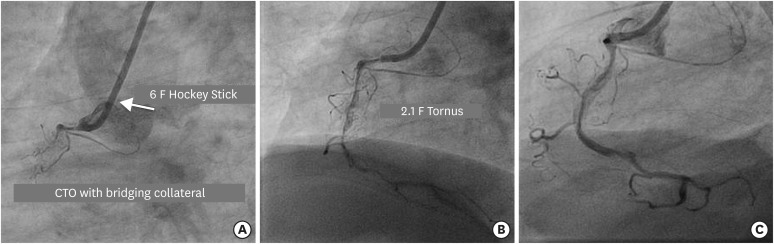
Figure 5 (A) Engagement of RCA ostium with 6 F Hockey Stick 4.0 guide catheter to address long segment CTO of ostio-proximal segment with bridging collateral. (B) Navigation of 2.1 F Tornus (in BU lesion) after Gaia 3 guidewire penetrates the proximal cap to be positioned in the distal true lumen. (C) Final result after spot stenting in long calcified lesion.BU = balloon-uncrossable; CTO = chronic total occlusion; RCA = right coronary artery.
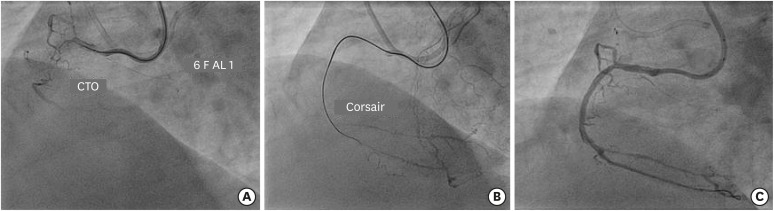
Figure 6 (A) Engagement of RCA ostium with 6 F AL 1guide catheter to address CTO of proximal segment with bridging collateral. (B) Facilitation of balloon crossing by Corsair microcatheter after Gaia 2 guidewire crosses the lesion. (C) Final result after deployment of 2 overlapping DES.CTO = chronic total occlusion; DES = drug-eluting stent; RCA = right coronary artery.
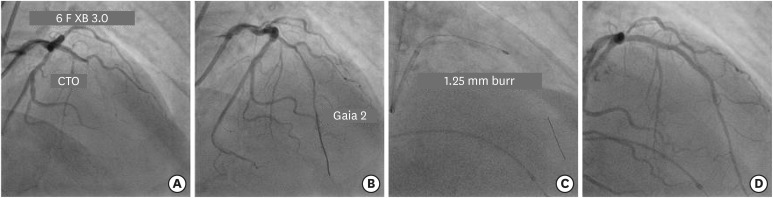
Figure 7 (A) Engagement of LMCA ostium with 6 F XB 3.0 guide catheter to fix long mid segment CTO of LAD. (B) Navigation of Gaia 2 guidewire across the occlusion into distal true lumen. (C) Rotational atherectomy with 1.25 mm burr to facilitate lesion crossing with balloon. (D) Final result after 2 overlapping DES.CTO = chronic total occlusion; DES = drug-eluting stent; LAD = left anterior descending; LMCA = left main coronary artery.
Reference
-
1. Stone GW, Reifart NJ, Moussa I, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part II. Circulation. 2005; 112:2530–2537. PMID: 16230504.2. Pagnotta P, Briguori C, Mango R, et al. Rotational atherectomy in resistant chronic total occlusions. Catheter Cardiovasc Interv. 2010; 76:366–371. PMID: 20839349.3. Stone GW, Colombo A, Teirstein PS, et al. Percutaneous recanalization of chronically occluded coronary arteries: procedural techniques, devices, and results. Catheter Cardiovasc Interv. 2005; 66:217–236. PMID: 16155889.4. Fang HY, Lee CH, Fang CY, et al. Application of penetration device (Tornus) for percutaneous coronary intervention in balloon uncrossable chronic total occlusion-procedure outcomes, complications, and predictors of device success. Catheter Cardiovasc Interv. 2011; 78:356–362. PMID: 21413119.5. Brilakis ES, Banerjee S. Crossing the “balloon uncrossable” chronic total occlusion: tornus to the rescue. Catheter Cardiovasc Interv. 2011; 78:363–365. PMID: 21976427.6. Von Sohsten R, Oz R, Marone G, McCormick DJ. Deep intubation of 6 French guiding catheters for tarnasradial coronary interventions. J Invasive Cardiol. 1998; 10:198–202. PMID: 10973341.7. Luna M, Papayannis A, Holper EM, Banerjee S, Brilakis ES. Transfemoral use of GuideLiner Catheter in complex coronary and bypass graft interevntions. Catheter Cardiovasc Interv. 2012; 80:437–446. PMID: 21805572.8. Ben-Dor I, Maluenda G, Pichard AD, et al. The use of excimer laser for complex coronary artery lesions. Cardiovasc Revasc Med. 2011; 12:69.e1–69.e8.9. Niccoli G, Giubilato S, Conte M, et al. Laser for complex coronary lesions: impact of excimer lasers and technical advancements. Int J Cardiol. 2011; 146:296–299. PMID: 21126783.10. Sueta D, Hokimoto S, Miyazaki T, et al. Usefulness of excimer laser atherectomy for balloon uncrossable lesion in chronic total occlusion. Int J Cardiol Heart Vasc. 2015; 9:70–72. PMID: 28785711.11. Patel SM, Pokala NR, Menon RV, et al. Prevalence and treatment of “balloon-uncrossable” coronary chronic total occlusions. J Invasive Cardiol. 2015; 27:78–84. PMID: 25661758.12. Michael TT, Banerjee S, Brilakis ES. Subintimal Distal Anchor Technique for “balloon-uncrossable” chronic total occlusion. J Invasive Cardiol. 2013; 25:552–554. PMID: 24088432.13. Han YL, Li Y, Wang SL, et al. Multi–wire plaque crushing as a novel technique in treating chronic total occlusions. Chin Med J (Engl). 2008; 121:518–521. PMID: 18364138.14. Li Y, Li J, Sheng L, et al. “Seesaw balloon-wire cutting” technique as a novel approach to “balloon-uncrossable” chronic total occlusions. J Invasive Cardiol. 2014; 26:167–170. PMID: 24717273.15. Liu R, Xu F, Liu T. Novel “crowbar effect” approach to improve success rate of recanalization of coronary chronic total occlusions. Technol Health Care. 2015; 23:S223–30. PMID: 26410487.16. Dash D. Retrograde coronary chronic total occlusion intervention using a novel reverse controlled antegrade and retrograde subintimal tracking. J Interv Cardiol. 2016; 29:70–74. PMID: 26728800.17. Dash D. Deja Vu of retrograde recanalization of coronary chronic total occlusion: A tale of a journey from Japan to India. Indian Heart J. 2016; 68:584–585. PMID: 27543488.18. Dash D. The retrograde recanalization of coronary chronic total occlusion: approaching through the backdoor. J Heart Lung Circ. 2017; 1:e104.19. Dash D. Problems encountered in retrograde recanalization of coronary chronic total occlusion: should we lock the backdoor in 2018? Indian Heart J. 2018; 70:132–134. PMID: 29455767.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thrombotic Occlusion during Intravascular Ultrasonography-Guided Percutaneous Coronary Intervention of Stumpless Chronic Total Occlusion
- Subintimal Tracking and Re-entry (STAR) Technique with Contrast Guidance for Chronic Total Occlusion: Experience with 4 Cases
- Polyarteritis Nodosa Complicated by Chronic Total Occlusion Accompanying Aneurysms on All Coronary Arteries
- Changes in Coronary Perfusion after Occlusion of Coronary Arteries in Kawasaki Disease
- Aspiration Thromboembolectomy in the Management of Acute Coronary Occlusion during Pertaneous Transluminal Coronary Angioplasty
