Dorsal-Plantar Loop Technique Using Chronic Total Occlusion Devices via Anterior Tibial Artery
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. cdhlyj@yuhs.ac
- KMID: 1503922
- DOI: http://doi.org/10.3349/ymj.2013.54.2.534
Abstract
- The effectiveness of below-the-knee (BTK) percutaneous transluminal angioplasty to obtain successful revascularization in patients with critical limb ischemia has been well established, and many of these patients with chronic lower-extremity disease have been treated by endovascular intervention as the firstline treatment. Dorsal-plantaer loop technique is one of the new BTK interventional techiniques, and includes recanalization of both pedal and plantar arteries and their anatomical anastomoses. This method generally needs two approaches simultaneously, including antegrade and retrograde. In this report, however, we describe a case in which dorsal-plantar loop technique with only one antegrade approach, using chronic total occlusion devices via anterior tibial artery, was used to successfully recanalize BTK arteries. We think that this new technique, which may represent a safe and feasible endovascular option to avoid more invasive, time-consuming, and riskier surgical procedures, especially in end-stage renal disease and diabetes, should be considered whenever the foot is at risk, and results of above-the-ankle percutaneous transluminal angioplasty remain unsatisfactory or insufficient to achieve limb salvage.
Keyword
MeSH Terms
Figure
-
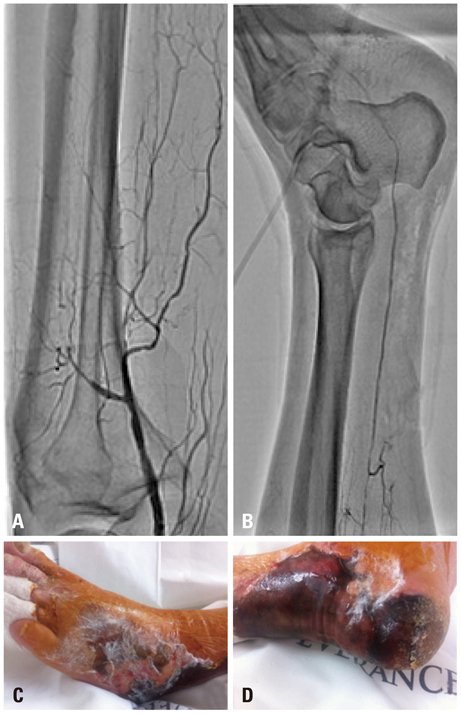
Fig. 1 Baseline peripheral angiography. (A) Baseline angiography revealed total occlusion of the left infrapopliteal artery with proximal portion of three distal run-off vessels. (B) The flow of distal posterior tibial artery and lateral plantar artery is shown. (C and D) A diffuse wound is distributed on the entire area of the foot including the transpedal puncture site.
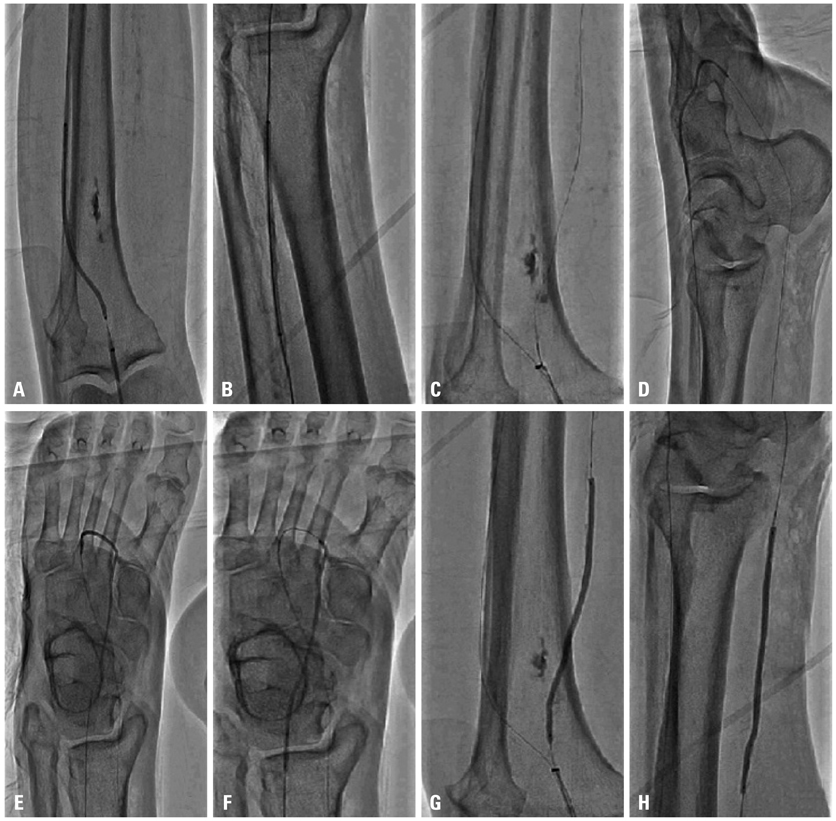
Fig. 2 Balloon angioplasty. (A and B) Balloon angioplasty of ATA using 3.0×100 mm EverCross balloon. (C) A 300-cm-long 014-inch hydrophilic guidewire was passed from ATA via a dorsal-plantar loop to PTA using the Corsair microcatheter. (D, E and F) Balloon angioplasty of dorsal-plantar loop (consisting of dorsalis pedis artery, deep plantar artery, deep plantar arch and lateral plantar artery) using 2.0×120 mm NanoCross balloon. (G and H) Balloon angioplasty of PTA using 3.0×100 mm EverCross balloon. ATA, anterior tibial artery; PTA, posterior tibial artery.

Fig. 3 (A-D) Final angiography. Final angiography reveals a well visualized anterior tibial artery, dorsal-plantar loop and posterior tibial artery with improved flow.
Reference
-
1. Carmona GA, Hoffmeyer P, Herrmann FR, Vaucher J, Tschopp O, Lacraz A, et al. Major lower limb amputations in the elderly observed over ten years: the role of diabetes and peripheral arterial disease. Diabetes Metab. 2005. 31:449–454.
Article2. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007. 45:Suppl S. S5–S67.
Article3. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006. 113:e463–e654.4. Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005. 366:1925–1934.
Article5. Söderström MI, Arvela EM, Korhonen M, Halmesmäki KH, Albäck AN, Biancari F, et al. Infrapopliteal percutaneous transluminal angioplasty versus bypass surgery as first-line strategies in critical leg ischemia: a propensity score analysis. Ann Surg. 2010. 252:765–773.
Article6. Reiber GE. The epidemiology of diabetic foot problems. Diabet Med. 1996. 13:Suppl 1. S6–S11.
Article7. Fusaro M, Dalla Paola L, Biondi-Zoccai G. Pedal-plantar loop technique for a challenging below-the-knee chronic total occlusion: a novel approach to percutaneous revascularization in critical lower limb ischemia. J Invasive Cardiol. 2007. 19:E34–E37.8. Fusaro M, Dalla Paola L, Brigato C, Marangotto M, Nicolini S, Rripay R, et al. Plantar to dorsalis pedis artery subintimal angioplasty in a patient with critical foot ischemia: a novel technique in the armamentarium of the peripheral interventionist. J Cardiovasc Med (Hagerstown). 2007. 8:977–980.
Article9. Manzi M, Fusaro M, Ceccacci T, Erente G, Dalla Paola L, Brocco E. Clinical results of below-the knee intervention using pedal-plantar loop technique for the revascularization of foot arteries. J Cardiovasc Surg (Torino). 2009. 50:331–337.10. Moore KL, Dalley AF. Clinically oriented anatomy. 1999. 4th ed. Philadelphia: Lippincott, Williams & Wilkins.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tourniquet Occlusion Technique for Infrapopliteal Artery Revascularization
- Calcified Anterior Tibial Artery Entrapment in Distal Third Tibial Fracture: A Case Report
- Drug-eluting Stent Implantation for a Below-the-knee Chronic Total Occlusion Lesion: A Case Report
- Novel Therapeutic Approach for Tibial Nerve Entrapment in Chronic Heel Pain Diagnosed as Plantar Fasciitis: A Case Report
- Restoring blood flow to the lateral plantar artery after elevation of an instep flap or medialis pedis flap
